Gynecologic Tumors, State-of-the-Art Michael A Bookman MD Chair, - PowerPoint PPT Presentation
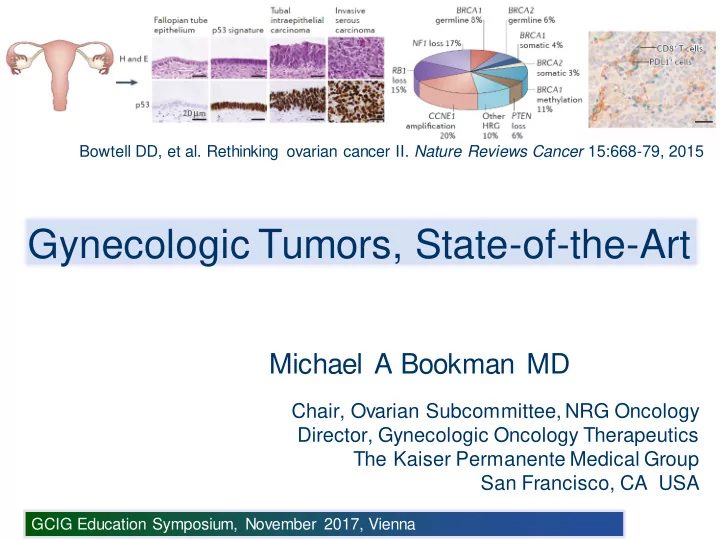
f Bowtell DD, et al. Rethinking ovarian cancer II. Nature Reviews Cancer 15:668-79, 2015 Gynecologic Tumors, State-of-the-Art Michael A Bookman MD Chair, Ovarian Subcommittee, NRG Oncology Director, Gynecologic Oncology Therapeutics The Kaiser
f Bowtell DD, et al. Rethinking ovarian cancer II. Nature Reviews Cancer 15:668-79, 2015 Gynecologic Tumors, State-of-the-Art Michael A Bookman MD Chair, Ovarian Subcommittee, NRG Oncology Director, Gynecologic Oncology Therapeutics The Kaiser Permanente Medical Group San Francisco, CA USA GCIG Education Symposium, November 2017, Vienna
Cervical Cancer: Global Mortality Global Mortality from Cervical Cancer exceeds 250,000 per year Ferlay J, et al. GLOBOCAN 2008 v2.0: International Agency for Research on Cancer GCIG Education Symposium, November 2017, Vienna
Cancer Evolution and Screening GCIG Education Symposium, November 2017, Vienna
High-Risk HPV Life Cycle Woodman BJ, et al. Nature Rev Cancer 2007; 7:11-22 GCIG Education Symposium, November 2017, Vienna
High-Risk HPV Antigen Expression Predominance of E6 and E7 with loss of capsid proteins (L1 and L2) Doorbar J, et al. Vaccine 2012;30S:F55-70 GCIG Education Symposium, November 2017, Vienna
Cervical Cancer: Interventions Cellular ? Neoadjuvant ? Adjuvant Immunity Surgery Alone Chemotherapy ChemoRx Vaccines Radiation Clinical +/- Concurrent Recurrence Staging Chemotherapy ? Fertility-Sparing or ? Vaginal Chemotherapy ? Dose- Risk-Stratified Surgery BrachyRT +/- anti-VEGF Schedule Prognostic factors • LVI, Stromal Invasion, Tumor Size, Hypoxia Immune • Histology, Demographics, PS Checkpoint • Access to Resources (daily radiation) Inhibition • Patterns of Spread • Pelvis, Distant Sites, Combined • Nodal vs Parenchymal vs Regional Extension GCIG Education Symposium, November 2017, Vienna
NCIC CTG CX.5: SHAPE A Randomized Trial Comparing Radical Hysterectomy and Pelvic Node Dissection vs Simple Hysterectomy And Pelvic Node Dissection in Patients with Low-Risk Early- Stage Cervical Cancer Low-Risk Cervical Cancer: • Stage IA2-IB1 squamous or adeno RADICAL Hysterectomy* I • T <2 cm, ≥3 mm intact cervical R stroma, <50% stromal invasion • Grade 1-3 SIMPLE Hysterectomy* II • No evidence of LN metastases (MRI) *Includes PLD (optional SLN) Stratified by Centers (SLN yes/no), Stage, Histology, Grade Post-operative adjuvant therapy permitted based on final pathology Primary Endpoint: Pelvic Relapse-Free Survival (PRFS) Non-inferiority design, p = 0.05, 80% power with one interim analysis Open: 01-DEC-2012 Plante M for NCIC CTG and GCIG-CCRN Target: 700 pts GCIG Education Symposium, November 2017, Vienna
Cervix NACT: INTERLACE • Stage IB2-IVA squamous or adenocarcinoma • Documented HIV negative • Excludes lower 1/3 vaginal invasion • Excludes LN metastases above aortic bifurcation Carboplatin AUC=2 Paclitaxel 80 mg/m 2 Standard CRT* (Weeks 1-6) R *40 to 50.4 Gy + weekly Cisplatin + ICBT Standard CRT* Stratified by Stage, LN status, Histology, T volume, Institution, IRMT (Yes/No) Primary Endpoint: Overall Survival p = 0.05, 80% power to detect a 10% increase in 5 year OS Open: NOV-2012 McCormack M for CRUK-NCRI and GCIG-CCRN Target: 630 pts GCIG Education Symposium, November 2017, Vienna
Impact of CTRT by Stage Clear benefit associated with Chemo-RT , but need for improved outcomes in high-risk disease Meta Analysis Collab. J Clin Oncol 26:5802-5812, 2008 GCIG Education Symposium, November 2017, Vienna
Cervix CRT: TACO GCIG/KGOG1027/TGCS2012: Randomized Phase III Clinical Trial Comparing Weekly vs Tri-weekly Cisplatin-Based Concurrent Chemoradiation in Locally-Advanced Cervical Cancer Radiation Therapy with • Stage IB2, IIB-IVA squamous Cisplatin 40 mg/m 2 ICBT or adenocarcinoma (Weekly x6) R Radiation Therapy with Cisplatin 75 mg/m 2 ICBT (Tri-Weekly x3) Primary Endpoint: Overall Survival p = 0.05, 80% power to detect a 10% increase in 5 year OS, HR = 1.50 Open: MAR-2012 Ryu for KGOG-ASGO and GCIG-CCRN Target: 590 pts GCIG Education Symposium, November 2017, Vienna
ANZGOG GOG0274: OUTBACK • Stage I-B1 PLN(+), I-B2, II, IIIB, IVA • GOG PS 0-2, HIV (-) • Squamous, Adenocarcinoma, or Adenosquamous • EBRT Dose (45 - 50.4 Gy) • Primary Endpoint: Overall Survival Carboplatin AUC=5 I Paclitaxel 155 mg/m 2 (3 h) x4 Concurrent Chemo-Radiation Cisplatin 40 mg/m 2 /wk R + Intracavitary Brachytherapy Observation II Open: 03-JAN-2012 Closed: 28-JUN-2017 (5.5 y) Accrual: 780 pts (increased to 900) Mileshkin L (ANZGOG), Moore K (NRG), et al. In progress GCIG Education Symposium, November 2017, Vienna
GOG 0240: Cervix (Advanced/Met) • Stage IV-B or recurrent with measurable disease • No prior chemotherapy, allow prior adjuvant RT+/-Chemo • Primary Objective: OS Cisplatin 50 mg/m 2 (d1 or d2) I Paclitaxel 135 or 175 mg/m 2 II +/- Bevacizumab 15 mg/kg Bifactorial Randomization 1. Chemotherapy 2. Bevacizumab Paclitaxel 175 mg/m 2 (3 h) Topotecan 0.75 mg/m 2 (d1,2,3) III IV +/- Bevacizumab 15 mg/kg DSMB Review JAN-2012: No evidence of superiority for non-Cisplatin regimen Open: 06-APR-09 Closed: 03-JAN-12 Accrual: 427 (eligible) Tewari KS, et al. NEJM 2014; 370:734-43 GCIG Education Symposium, November 2017, Vienna
GOG 0240: Cervix (Advanced/Met) Overall Survival Progression-Free Survival 1.0 1.0 HR (+/- 95% CI) = 0.67 (0.54-0.82) HR (+/- 97% CI) = 0.71 (0.54-0.95) 0.8 0.8 p = 0.0002 (2-sided) p = 0.0035 (1-sided) Median: 8.2 vs 5.9 months Median: 17.0 vs 13.3 months 0.6 0.6 Chemo + Bev (n = 227) Chemo + Bev (n = 227) 0.4 0.4 Chemo Alone (n = 225) 0.2 0.2 Chemo Alone (n = 225) 0.0 0.0 0 12 24 36 0 12 24 36 Months on Study Months on Study FDA approved indication for bevacizumab with chemotherapy 14-AUG-2014 Tewari KS, et al. NEJM 2014; 370:734-43 GCIG Education Symposium, November 2017, Vienna
GOG0240: Fistula Complications Chemo+Bev Chemo (n=218) (n=222) GI-vaginal fistula 18 ( 8.2%) 2 (0.9%) GU-vaginal fistula 4 ( 1.8%) 3 (1.4%) GI fistula (other) 1 ( 0.5%) 0 ( 0%) T otal Fistula 23 (10.5%) 5 (2.3%) Perforation / Peritonitis 8 ( 3.6%) 0 ( 0%) • Fistula risk increased with bevacizumab, particularly after prior radiation • Patient treatment decisions need to be individualized Willmott LJ, et al. IGCS 2015 GCIG Education Symposium, November 2017, Vienna
Activating Cellular Immunity Some Lm -LLO is killed and degraded within Lm , Listeria monocytogenes the phagolysosome TAA, tumor-associated antigen tLLO, truncated listeriolysin O AXAL, Axalimogene Filolisbac Lm -LLOis phagocytosed by APC Peptide-MHC APC complexes stimulate CD4+ (MHC II) and CD8+ (MHC I) T cells Some Lm -LLO escapes the phagolysosome and enters the cytosol Proteasomal degradation of tLLO-TAA fusion protein into peptides for MHC class I Ag presentation Modified from: Advaxis Immunotherapies GCIG Education Symposium, November 2017, Vienna
AXAL Adjuvant Monotherapy GOG-3009 (Advaxis ADXS001-02) Open: 03FEB2017 Target: 450 patients Herzog T. for GOG-Foundation GCIG Education Symposium, November 2017, Vienna
Cervical Cancer: Anti-PD-L1 Total n = 24, Squamous n = 23 KEYNOTE-028 (NCT02054806) Phase IB Multicohort Frenel J-S, ASCO 2016 GCIG Education Symposium, November 2017, Vienna
GOG3016: Anti-PD1 vs ChemoRx • Fully human hinge-stabilized IgG4P, binds to human PD-1 ECD • Cervical Cancer, progression or recurrence < 6 m from prior platinum-based therapy (platinum-refractory) • Stratification by histology, geographic region, prior bevacizumab • Endpoints: OS (Primary), PFS and ORR (Secondary) REGN2810 I 350 mg IV q3w (x8 cycles) R Chemotherapy II Investigator’s Choice* * Pemetrexed, topotecan, irinotecan, Vinorelbine, gemcitabine Open: SEP2017 Accrual: 436 pts GOG Foundation (under development) GCIG Education Symposium, November 2017, Vienna
Cervical Cancer • Universal multivalent HPV vaccination to prevent infection in children, with an emphasis on high-risk populations in the developing world • Development of low-resource strategies for HPV vaccination and screening • Potential to activate the cellular immune response using novel E6/E7 vaccines • Tailored management of early-stage disease, including minimized surgery (SHAPE) • Optimized management of high-risk disease, including adjuvant chemotherapy, dose/schedule of cisplatin • Prospective randomized evaluation of NACT (INTERLACE) • Improved PFS and OS following incorporation of bevacizumab with chemotherapy for metastatic or recurrent disease, but with an increased risk of fistula formation (in patients with prior radiation) • Evaluation of immune checkpoint inhibition in high-risk and advanced disease GCIG Education Symposium, November 2017, Vienna
Obesity Trends, US (BMI ≥30) 1985 1990 1995 2000 2005 2006 No Data <10% 10% – 14% 15% – 19% 20% – 24% 25% –29% ≥30% Source: CDC Behavioral Risk Factor Surveillance System GCIG Education Symposium, November 2017, Vienna
Metformin Translational Window New Diagnosis BMI ≥30 Metformin Definitive Surgery Endometrioid Histology 850 mg QD (within 7-28 d) • Tissue microarrays pre- and post-metformin • Immunohistochemistry Ki-67, pAMPK, mTOR, pAKT, pS6, ER/PR • Metabolomics panel (serum and tissue) Pre-Rx Post-Rx Mean Ki-67 Index Pre-Rx: 39.5 Post-Rx: 27.7 (n = 20) IHC Molecular Markers (Pre- and Post-Rx) 60.3% 44.2% pS6 51.2% pAMPK pAKT p4EBP1 74.7% ER 65.7% PR (NC) Schuler KM, et al. SGO 2014 (Abstract 8) GCIG Education Symposium, November 2017, Vienna
Recommend




More recommend
Explore More Topics
Stay informed with curated content and fresh updates.