
SLIDE 1
1
Gastrointestinal Lymphomas
EATL, MALT, and beyond Maria A. Pletneva, MD, PhD
Lymphoma in GI tract
- Uncommon compared to GI epithelial neoplasms
- 20% of all lymphomas occur in the GI tract
- B‐cell lymphomas are far more common than T‐
cell lymphomas
- Most common lymphoma in GI tract is diffuse
large B‐cell lymphoma
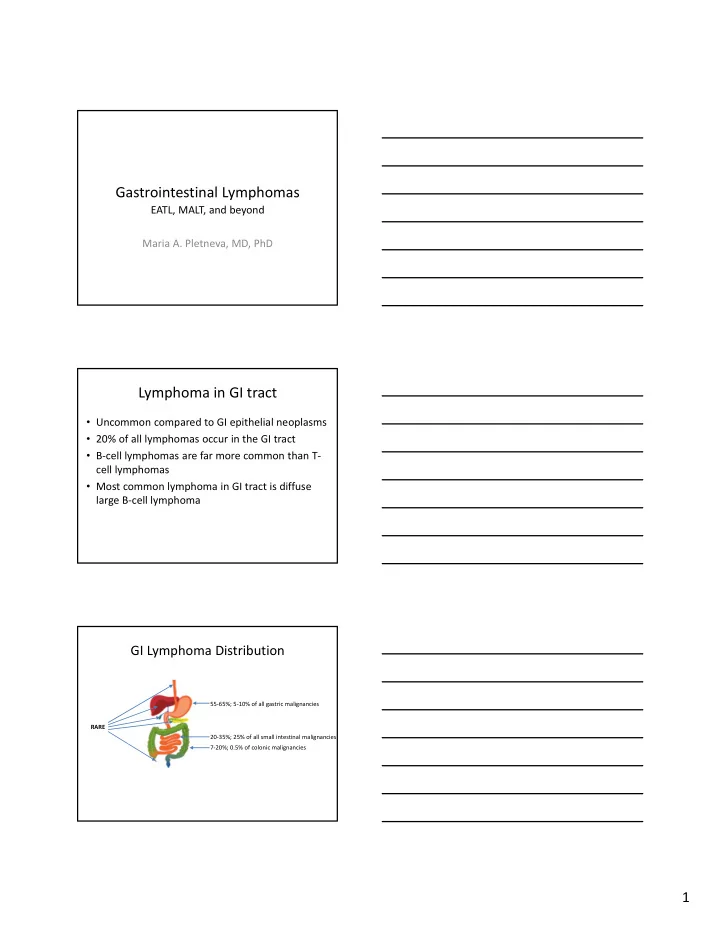
GI Lymphoma Distribution
RARE 55‐65%; 5‐10% of all gastric malignancies 20‐35%; 25% of all small intestinal malignancies 7‐20%; 0.5% of colonic malignancies