DRAFT 19 October 2017 Please do not Cite. Results are preliminary. - PDF document
DRAFT 19 October 2017 Please do not Cite. Results are preliminary. Background Paper to accompany poster at IUSSP Cape Town 2017 Fertility Responses to Child Deaths in Historical and Contemporary Populations George Alter, University of Michigan
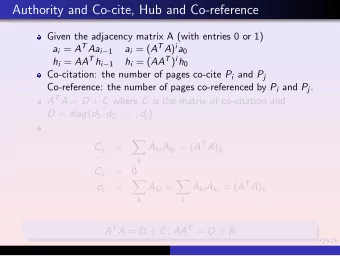
DRAFT 19 October 2017 Please do not Cite. Results are preliminary. Background Paper to accompany poster at IUSSP Cape Town 2017 Fertility Responses to Child Deaths in Historical and Contemporary Populations George Alter, University of Michigan Estelle McLean, London School of Hygiene and Tropical Medicine and Malawi Epidemiology and Intervention Research Unit Aisha N.Z. Dasgupta, United Nations Population Division and London School of Hygiene and Tropical Medicine Descriptions of fertility transitions in Europe generally assume that birth control was used to avoid exceeding a desired family size. This implies that couples who suffered a child death would have been less likely to practice birth control than couples whose children survived. From this perspective the emergence of a “replacement effect” (i.e. higher fertility following a child death) is a sign of the practice of family limitation. Knodel (Knodel 1982; 1988) found much stronger evidence of a replacement effect among German village populations after fertility began to decline. Ethnographic research on Africa has encountered a very different response to child deaths. Bledsoe, Banja, and Hill (1998) describe a mother who began using modern birth control following the death of her child in spite of a strong desire for more children. Concerned that repeated pregnancies were eroding her capacity for childbearing, this woman believed that rest and recuperation were the best way to assure that her next pregnancy would be successful. The use of modern contraception for birth spacing has important implications for understanding the slow pace of fertility decline in Africa. As some observers predicted (Caldwell, Orubuloye and Caldwell 1992), fertility in African societies seems to be following a very different path than Europe and East Asia. This paper will look for the contrasting responses to child deaths described by Knodel and Bledsoe. Birth intervals have been reconstructed from a subset of Knodel’s German village genealogies which we contrast with data from the Karonga Health and Demographic Surveillance Site in northern Malawi. Our analysis employs the “split population” or “cure model,” a mover/stayer model in which covariates can have separate effects on “stopping” and “spacing” (Kuk and Chen 1992; Li and Choe 1997; Yamaguchi and Ferguson 1995). Since infant deaths tend to increase fertility by terminating breastfeeding, the estimation model uses time-varying covariates for child deaths and time since last birth. Two Models of Fertility and Birth Control We characterize Knodel’s (1982) description of the emergence of a child replacement effect as an extension of the “natural fertility hypothesis” proposed by Louis Henry (Henry 1961). H enry’s model emphasizes the shift to parity-dependent fertility control, which implies that couples begin aiming for a target family size. In this framework we
DRAFT 19 October 2017 Please do not Cite. Results are preliminary. expect a child replacement effect to emerge with the transition to family limitation. If fertility behavior is not being affected by family size, we do not expect behavior to change after the death of a child. We also examine other implications of the Natural Fertility Hypothesis, such as the prediction that fertility transitions occur because of ‘stopping’ rather than ‘spacing’ (Knodel and van de Walle 1979). Caroline Bledsoe and her co-authors have offered a very different description of fertility decisions of African women. Bledsoe, Banja, and Hill (1998) describe a mother who began using modern birth control following the death of her child in spite of a strong desire for more children. Concerned that repeated pregnancies were eroding her capacity for childbearing, this woman believed that rest and recuperation were the best way to assure that her next pregnancy would be successful (Bledsoe et al. 1998; Bledsoe and Banja 2002). Thus, modern contraception can be used with the intention of increasing rather than limiting family size. Bledoe’s (2002) account emphasizes the belief that a woman’s physical capacity for childbe aring is limited and that adverse events, such as miscarriages and infant deaths, deplete her strength and endanger the survival of the next birth. Women may reach a point where they retire from childbearing, because they believe themselves unable to successfully bear another child. This decision is based on an evaluation of their physical condition, and it does not reflect a desire to stop after a target family size has been reached. We call this the “Bodily Expenditure Hypothesis.” Data Data for this paper come from historical and contemporary sources. We use family reconstitutions for six German villages collected by John Knodel from village genealogies (Knodel 1988). Fertility in rural Germany began to decrease in the last quarter of the nineteenth century. Most of these villages were predominantly Catholic, but there are two Protestant villages and one with Jews. Our analysis is limited to couples who were both married for the first time. Table A1 shows numbers of births, person-years at risk, and age-specific marital birth rates for the German village sample. The total marital fertility rate in this sample decreases from 8.6 in 1800-1850 to 4.6 after 1925. We also analyze data from the health and demographic surveillance system in Karonga District in rural northern Malawi. The Karonga HDSS grew out of earlier projects to control infectious diseases (Crampin et al. 2012; Jahn et al. 2007). Data from annual interviews and a network of trained village informants are available from 2002 to 2015. Christianity is the primary religion in Karonga (Baschieri et al. 2013). Our analysis is limited to women who were currently in a union, as indicated by reports about marital status, partners, and co-residence. Divorce was common in Karonga, and we include all time that women were in a union. We also include women in polygamous marriages, who account for about 22 percent of the time under observation. Table A2 shows numbers of births, person-years at risk, and age-specific marital birth rates for the
DRAFT 19 October 2017 Please do not Cite. Results are preliminary. Karonga HDSS. The total fertility of women in unions decreased from 6.7 in 2002-2007 to 6.1 in 2008-2015. Our regression analysis is limited to women who have had at least one birth, and it is stratified by time period and number of previous births (parity). Tables A3 and A4 show person-years at risk by time period and parity in each sample. We use three time-varying covariates to measure the effect of child deaths on fertility, which are depicted in Figure 1 . Breastfeeding reduces fertility by delaying a woman’s return to ovulation. An infant death terminates breastfeeding prematurely and results in an earlier pregnancy, unless the couple is using birth control. To distinguish between the effect of lactation on fertility, we separate the impact of a child death into three periods: 9 to 21, 21 to 33, and 33 to 56 months after the previous birth. If an infant dies, we expect fertility to rise with a nine-month lag. We also expect the impact of lactation to be stronger in the first year after a birth than in the second year. Thus, if an infant dies at age 4 months, we expect fertility to rise 13 months after the birth. We also expect the effect breastfeeding to be greater in the first than in the second year of life. So, we use one variable to measure the effect of ending lactation during the first 12 months of a child’s life (Infant death 1 -12 months), and a second variable to measure the effect of ending lactation on fertility during the second year of life (Infant death 13-24 months). In both cases the effect on fertility is lagged by 9 months. Both infant death variables describe effects of the most recent child, and they are reset when another child is born. We use a separate variable (Child death) to measure effects of child deaths that are not related to lactation. To avoid confusing this effect with lactation, this variable takes effect from 33 (i.e. 2 4+9) to 56 months after the child’s birth, when we expect the impact of lactation on fertility to be minimal. Unlike the infant death variables, the child death variable is not reset after each birth. Since this variable is intended to detect a child replacement effect, the death of the first child should increase motivation for another birth even after the second child is born. Figure 1. Periods Covered by Time-varying Covariates for Child Deaths Months since last birth 0- 3- 6- 9- 12- 15- 18- 21- 24- 27- 30- 33- 36- 39- 42- 45- 48- 51- 54- 2 5 8 11 14 17 20 23 26 29 32 35 38 41 44 47 50 53 56 Infant death 1-12 Infant death 13-24 Child death
Recommend






![Draft Benzo[a]pyrene Charge Question Responses 1 Revised Draft Responses to Charge Questions](https://c.sambuz.com/668898/draft-benzo-a-pyrene-charge-question-responses-s.webp)


More recommend
Explore More Topics
Stay informed with curated content and fresh updates.