11/21/2017 Do it Yourself: Home Exercise for Lower Extremity Problems Katie Elston ATC; Elise Hammond ATC; Derek Hirai, MS, ATC 1 Disclosures We have nothing to disclose. 2 1
11/21/2017 What is an Athletic Trainer? 3 What is an Athletic Trainer (AT)? Allied Health Care Professional Domains • Prevention • Evaluation • Immediate Care • Treatment, Rehab, Reconditioning • Organization and Administration • Professional Responsibility 4 2
11/21/2017 AT Clinical Responsibilities at UCSF 5 Presentation Goals Provide basic instruction of LE acute injury care Understand the importance of acute injury care Understand the goals of early phases of rehab 6 3
11/21/2017 Goals of Acute Injury Care Minimize further damage Reduce hemorrhage and edema Relieve pain and spasm Promote healing (Baoge 2012) 7 Injury Process Inflammatory Phase • 1-4 days post injury Proliferation Phase • 2-4 days post injury • Can last up to 6 weeks Remodeling Phase • Starts after at least 3 weeks post injury • Requires 12 months to become maximal (Baoge 2012) 8 4
11/21/2017 Inflammatory Phase Immediate onset tissue death Hematoma formation Inflammatory cells • Leukocytes • Macrophages (Baoge 2012) 9 Proliferation Phase New tissue laid down Injury site contracts as new tissues are built Blood vessels rebuilt 10 5
11/21/2017 Inflammatory Phase P rotection R est I ce C ompression E levation Minimum 2-3 days post injury! 11 Proliferation Phase Improve/maintain range of motion Limit loss/maintain muscle strength and coordination Continue to promote an ideal healing environment 12 6
11/21/2017 Thigh Injuries Muscle strain • Quadriceps, hamstring, hip flexor Muscle contusion Differential diagnoses 13 Thigh Muscle Strain MOI = Eccentric loading of muscle fibers (Boublik 2013) Causes tearing of muscle or tendon fibers R/o muscle avulsion injury 14 7
11/21/2017 Sports Related Hamstring Strain 15 Thigh Muscle Contusion “Charley Horse” MOI = blunt force trauma (Kary 2010) Causes tearing of muscle fibers R/o fracture 16 8
11/21/2017 Differential Diagnoses Compartment Syndrome • Direct trauma • Life/limb threatening (Burns 2004) Osteochondritis Dissecans Acute Fracture • Direct trauma • Avulsion fracture during eccentric loading (adolescent athletes) Muscle Cramp Radiculopathy 17 PRICE - Protection Typically thigh injuries do not require any type of DME 18 9
11/21/2017 PRICE - Rest Remove from activity to prevent further injury Consider assistive walking devices to limit pain, improve mobility, prevent secondary injury, decrease risk of falling 19 PRICE - Ice Ice for 15-20 minutes every 1-2 hours Always use a towel or thin barrier to protect skin Never sleep with ice applied to the body 20 10
11/21/2017 PRICE - Compression Elastic wrap over the injured area. For muscle contusions, use foam pad with elastic wrap to minimize hematoma development. Consider adding a compression stocking if patient develops lower leg edema. 21 PRICE - Elevation Elevate injured area above heart. Combine elevation with compression and/or ice 22 11
11/21/2017 Initial Rehab Exercises Goals of early intervention: • Decrease swelling • Decrease pain • Restore range of motion • Restore strength • Restore neuromuscular control 23 Stretching Early static stretching encourages elongation of maturing scar tissue (Kary 2010) Hamstring Stretching Quadriceps Stretching 24 12
11/21/2017 Strengthening Early muscle activation reduces strength losses (Slider2013) Isometric concentric eccentric Flex Hamstring Isometrics Quadriceps Isometrics 25 Thigh Injuries Wrap-Up Can become a chronic issue due to poor treatment and/or rehab Consider referral to physical therapy Educate patient to return to activity slowly 26 13
11/21/2017 Ankle Injuries Ankle sprains are one of the most common musculoskeletal injuries occurring in sports and sedentary persons. (Fong DT, 2008) The rate of ankle sprains can occur from 15-20% of all sports injuries. (Aiken, 2008) 77% of all ankle sprains are lateral ankle sprains. Most occur during ankle inversion and plantar flexion. 27 Ankle Sprain Classifications Grade 1 • Mild stretching of ligament complex w/o joint instability, weight bearing, no hemorrhaging Grade 2 • Partial rupture of the ligament complex with mild instability, hemorrhaging, tender to palpate, some loss of function Grade 3 • Complete rupture of the ligament complex with joint instability, Hemorrhaging, great loss of normal function, 28 14
11/21/2017 Sports Related Ankle Sprain 29 Non-Sports Related Ankle Sprain 30 15
11/21/2017 Differential Diagnosis Syndesmosis sprain = high ankle sprain • Occurs in 1-24% of ankle sprains • If disrupted, may need surgical intervention Fracture • Medial or lateral malleolus, base of 5th metatarsal, or navicular • Refer to Ottawa Ankle Rules Lis Franc fracture/dislocation • Disruption of the TMT ligaments at the TMT joint Osteochondral lesion of talus • Persistent pain and swelling Achilles rupture 31 Which one is fractured? 32 16
11/21/2017 Ottawa Ankle Rules 33 PRICE - Protection Consider prescribing a brace or Air Cast walking boot Grade I and II lateral ankle sprains • Decreased pain/swelling (Kerkhoff et al. 2001) • Reduced time off from work/sport compared to using elastic wrap (Beynnon et al. 2006) Grade III lateral ankle sprains • Clinical consensus suggests Walking Boot that some form of immobilization is necessary (NATA 2013, Lamb et al. 2009) 34 17
11/21/2017 PRICE - Rest Remove from activity to prevent further injury Consider assistive walking devices to limit pain, improve mobility, prevent secondary injury, decrease risk of falling 35 PRICE - Ice Ice for 15-20 minutes every 1-2 hours Always use a towel or thin barrier to protect skin Never sleep with ice applied to the body 36 18
11/21/2017 PRICE - Compression Elastic wrap or compression stocking over the foot and ankle. 37 PRICE - Elevation Elevate injured limb above heart Combine elevation with compression and/or ice 38 19
11/21/2017 Initial Rehab Exercises Goals of early intervention: • Decrease swelling • Decrease pain • Restore range of motion • Restore strength • Restore neuromuscular control 39 Range of Motion – Ankle Pumps Goal: Restore and maintain ankle plantar flexion and dorsiflexion Frequency: 2 sets 15, 3 times/day 40 20
11/21/2017 Range of Motion – ABC’s Goal: Restore and maintain ankle motion Frequency: 2 sets A-Z, 3 times/day 41 Range of Motion – ABC’s Goal: Restore and maintain ankle motion Frequency: 2 sets A-Z, 3 times/day 42 21
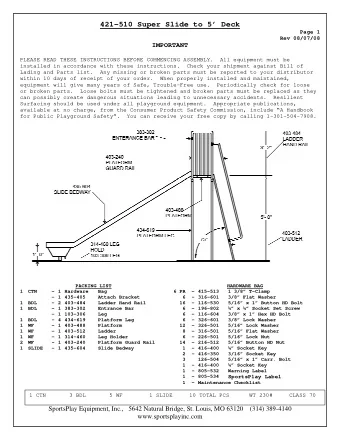
ACUTE ANKLE INJURY PROTOCOL For instructional videos of this protocol, visit sportsrehab.ucsf.edu BACKGROUND: Sw elling Reduction • Use an ACE WRAP to reduce swelling around your ankle. o Start at your toes and wrap half way up your lower leg. o Tension should be tighter around your toes and loose on your leg. • Wear your wrap 24/7. • Remember to elevate you ankle above your heart to encourage a decrease in swelling Cold Therapy • Ice injured ankle 15 min every 2 hours. • Ice packs should be combined with elevation of the ankle. • Place a hand towel or cloth napkin between the skin and the ice. • Continue Ice Therapy until swelling resolves. INCREASE RANGE–OF-MOTION: START NOW Ankle Pumps Point foot away from body, curl toes. Pull foot toward body, extend toes. Speed doesn’t matter. Slow steady pace. Frequency : 2 sets x 15reps 3 times per day. Goal : Increase Plantar/Dorsi Flexion of the Ankle Ankle Alphabet Imagine your big toe as a pencil. Trace the capital letters of the alphabet. Use big, loopy, motions. Frequency : 2 sets, A-Z. 3 times per day. Goal : Increase All Motions of the Ankle Calf Stretching Start in a seated position Place towel over ball of the foot Gentle pull ankle back to stretch calf Frequency : 3 sets x 2 min. 3 times per day. Goal : Increase All Motions of the Ankle FOOT STRENGTH Tow el Toe Pulls Use a medium sized towel. Place a 1 lb weight at the end. Use toes to grab towel and pull it toward you. Repeat FIVE Times. Frequency : 1 set. 3 times per day. Goal : Increase Strength of Toe/Foot Flexors UCSF Orthopaedic Institute | 1500 Owens Street Ste 170 | San Francisco, CA 94158 | Phone: 415-353-2808 | Fax: 415-353-7593 | orthosurg.ucsf.edu
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries