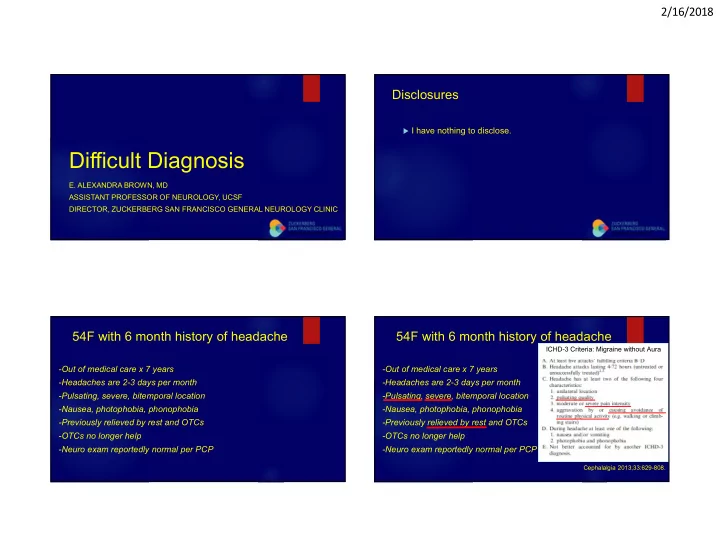
2/16/2018 Disclosures I have nothing to disclose. Difficult Diagnosis E. ALEXANDRA BROWN, MD ASSISTANT PROFESSOR OF NEUROLOGY, UCSF DIRECTOR, ZUCKERBERG SAN FRANCISCO GENERAL NEUROLOGY CLINIC 54F with 6 month history of headache 54F with 6 month history of headache ICHD-3 Criteria: Migraine without Aura -Out of medical care x 7 years -Out of medical care x 7 years -Headaches are 2-3 days per month -Headaches are 2-3 days per month -Pulsating, severe, bitemporal location -Pulsating, severe, bitemporal location -Nausea, photophobia, phonophobia -Nausea, photophobia, phonophobia -Previously relieved by rest and OTCs -Previously relieved by rest and OTCs -OTCs no longer help -OTCs no longer help -Neuro exam reportedly normal per PCP -Neuro exam reportedly normal per PCP Cephalalgia 2013;33:629-808. 1
2/16/2018 54F with 6 month history of headache 54F with 6 month history of headache ICHD-3 Criteria: Migraine without Aura -Out of medical care x 7 years -Out of medical care x 7 years -Headaches are 2-3 days per month -Headaches are 2-3 days per month -Pulsating, severe, bitemporal location -Pulsating, severe, bitemporal location -Nausea, photophobia, phonophobia -Nausea, photophobia, phonophobia -Previously relieved by rest and OTCs -Previously relieved by rest and OTCs -OTCs no longer help -OTCs no longer help -Neuro exam reportedly normal per PCP -Neuro exam reportedly normal per PCP Cephalalgia 2013;33:629-808. Red flags Neurology consultation further details What features should worry you about secondary headache? ∙ Awakens from sleep with occipital headache x 1 year ∙ No previous headache history -Systemic symptoms (fevers, chills, weight loss, HIV, cancer) ∙ Born in Mexico -New headache in an older patient >50 y.o. ∙ Has not been taking any medications for HA -Abrupt onset reaching maximum intensity in < 1 minute ∙ Neurological exam reveals right dysmetria -Exacerbated by positioning or Valsalva -Abnormal neurological/fundoscopic exam MRI brain with and without Gad was performed Nye BL, Ward TN. Headache 2015 Oct: 1301-1308. 2
2/16/2018 Neurocysticercosis CNS infection by larval form of pork tapeworm Taenia solium Most common helminthic CNS infection A leading cause of acquired epilepsy worldwide Clinical presentation depends on: Location of cysts Stage of parasite Host immune response T1 T2 FLAIR Post Gad T1 Garcia HH, et al. Lancet Neurol. 2014;13: 1202-15. Endemic regions Q1: How do humans become infected with neurocysticercosis? A. Eating undercooked pork containing viable 46% cysticerci B. Ingesting food or water contaminated with 33% human feces containing T. solium eggs 19% C. Ingesting food or water contaminated with porcine feces containing T. solium eggs D. Transmission through blood from an infected 2% 0% person . e . . . . . . . v i . . . . o E. None of the above v d d n i b g e e a n a t a t a i n n m e n h a i m i m i o t t r f n a a f o o t t d e c n n o n o o o k c c l o r r r b N o e e h p t t d a a u g e w w o k r r r o o o h o d d t c o o n e r o d o o i f f s n g g s i u n n m Garcia HH, et al. Lancet Neurol. 2014;13: 1202-15. g t i t i s n s s n e e a t i g g a n n T r E I I 3
2/16/2018 Life cycle of Taenia solium Life cycle of Taenia solium Taeniasis: 1 parasite, ∙ Adult tapeworm 2 infections infection Taeniasis ∙ Human eats undercooked pork and containing viable Cysticercosis cysticerci Kraft R. Am Fam Physician. 2008 Mar 15;77(6):748. Kraft R. Am Fam Physician. 2008 Mar 15;77(6):748. T. Solium Cyst Stages of Development Life cycle of Taenia solium Cysticercosis: Vesicular Granular nodular Colloidal Calcified ∙ Viable ∙ Begins Degeneration ∙ Degenerates further ∙ Dead ∙ Infection caused by larval ∙ Non-enhancing ∙ Ring enhances ∙ Ring enhances ∙ Punctate Ca 2+ stage of tapeworm T. ∙ Scolex=“hole-with-dot” ∙ +/- Scolex ∙ No Scolex ∙ No Scolex solium ∙ No edema ∙ Less edema ∙ Edema ∙ Minimal/No Edema Garcia. Lancet Neurol. 2014;13: 1202-15. Del Brutto OH. Scientific World Journal 2012;2012:159821. Sinha S, et al. Journal of Clinical Neuroscience 2009;16: 867-76. Kraft R. Am Fam Physician. 2008 Mar 15;77(6):748. Zhao JL, et al. Radiology of Infectious Disease 2015;1:94-102. 4
2/16/2018 NCC brain locations Subarachnoid NCC Excessive T. solium larval growth enlarged multiloculated cysts ( racemose =“bunch of grapes”) MRI spine should be performed in basal subarachnoid NCC High risk asymptomatic spinal cord Parenchymal Extraparenchymal involvement. If present treat surgically Intraventricular (usually 4 th ventricle) Usually gray-white junction (consensus) Subarachnoid (basal cisterns, sylvian fissure) Can manifest as seizures Can manifest as hydrocephalus, focal neurological deficits, complications of ↑ ICP Callacondo et al. Neurology 2012;78(18):1394-1400. Garcia HH, et al. Clin Microbiol Rev 2002;15:747-56. Sinha S, Sharma BS. Journal of Clinical Neuroscience 2009;16: 867-76. Diagnostic Criteria for NCC Immunological Diagnosis Imaging EITB assay (Western Blot): TEST OF CHOICE (MAINSTAY) ELISA based assay Dx Exposure Clinical Hx Presentation Serologic Testing Gripper. Acta Tropica 2017;166:218-224. 5
2/16/2018 Q2: What is the next step in this Subretinal cysts patient’s care? Dilated eye exam is essential prior to initiating Albendazole or Praziquantel A. Start antihelminthic therapy with Albendazole 15 Antihelminthic therapy provokes inflammatory response around dying cysticerci 72% mg/kg/day for a minimum of 10 days can lead to blindness B. Start steroid therapy with Dexamethasone 0.1 Surgical removal of cyst is treatment of choice for ocular cysts (consensus) mg/kg/day then administer Albendazole 15 mg/kg/day for a minimum of 10 days C. No indication for antihelminthic therapy given that the 15% 7% 6% appearance of these cysts does not warrant antihelminthic drugs . . . . D. Do not initiate antihelminthic therapy until further . . . . . y . . . n h i i p h m t a t n r i l i e w e m h h y i e l t p t h workup is performed c n i a a i h r n t t e r Del Brutto OH, et al. Journal Neurol Sci 2017;372:202-10. n h o a t f m i e d n t l i o a e o i i h r t t i e a n i Kori P, et al. Neurology 2013;81:135-6. t t c n s i i a d t t n o t r n r a i a t o o t S N D Padhi TR, et al. Survey of Ophthalmology 2017;16:161-89. S Q3: Which antihelminthic drug regimen is Antihelminthic drugs appropriate for a patient with NCC whose brain imaging is notable for >3 calcified cysts? Albendazole 15 mg/kg/day x 7-10 days A. 56% Albendazole, Praziquantel - Used to treat viable cysts Albendazole 22.5 mg/kg/day x 7-10 days B. C. Combination therapy Albendazole 15 mg/kg/day x 7-10 31% Not used for calcified cysts which are already dead days + Praziquantel 50 mg/kg/day x 7-10 days Worsened inflammation during cyst destruction temporarily worsens symptoms D. Concurrent treatment of Dexamethasone 0.1 mg/kg/day 10% 1% 2% Must control symptoms first (if needed, undergo lesion resection, ventricular with Albendazole 15 mg/kg/day x 7-10 days to control shunt placement, steroids, etc) There is no rush to initiate antihelminthic drugs! intracranial inflammation s s e y y v a a . . . o d d . . . b 0 5 1 a a 0 h 1 1 e e t e 7 - 7 - o l m h None of the above x t x a z a f E. y y d x o a a n e e Give steroids simultaneously to control inflammation d d e D n / / b o g g l o f N k k A g / g / t m m p y n m e 5 5 a 1 . e r t 2 h a e 2 t e Gripper. Acta Tropica 2017;166:218-224. o l n t r z l e o a o i n t d z t e n a a r e d n r b n b i u Garcia HH, et al. Clin Inf Dis 2016;62: 1375-79. l e m c A b n A l o o C C 6
2/16/2018 Back to our case Steroids were initiated right away Dexamethasone 4 mg TID x 3 days, T2 FLAIR at 4 months then 2 mg TID x 2 weeks, then Prednisone 0.4 mg/kg daily T2 FLAIR at 15 months Clinic follow-up: headaches resolved, R dysmetria resolved Ophthalmology: no intra-ocular cysticercosis Spine MRI with and without Gad: no cysticerci Cysticercosis IgG Ab: 3.77 H (>0.51 is positive) Alongside Prednisone, administered Albendazole 15 mg/kg/day x 4 weeks INITIAL T2 FLAIR Ca+Vit D, Famotidine while receiving steroids Return precautions given; patient closely monitored, remained asymptomatic Take home points Thank you Antihelminthic drug treatment is NEVER the main priority, rather first address patient’s symptoms (seizures, increased ICP). There is no rush to begin antihelminthic drugs. Pay attention to cyst stage: there is no role for antihelminthic drugs if only calcified lesions are seen . Obtain dilated eye exam prior to initiating antihelminthic drugs; subretinal cysticerci should be surgically resected. Administer steroids alongside antihelminthic drugs to limit inflammation that occurs with dying cysts. Happy to answer questions Garcia HH, et al. Clin Microbiol Rev 2002;15:747-56 . 7
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries




![Ice and Stride [ a ] Common User Complaints Common User Complaints Difficult to Ice Specific](https://c.sambuz.com/726487/ice-and-stride-a-common-user-complaints-common-user-s.webp)