Clinical Challenge Clinical Challenge Possible Causes: - PDF document
Disclosure-of-Relationship Role of Pre-procedure Imaging Before VT - Research Grants Biosense-Webster, Ablation Just Pretty Pictures or Critical General Electric Information to Guide Ablation? - 7th Annual California Heart Rhythm
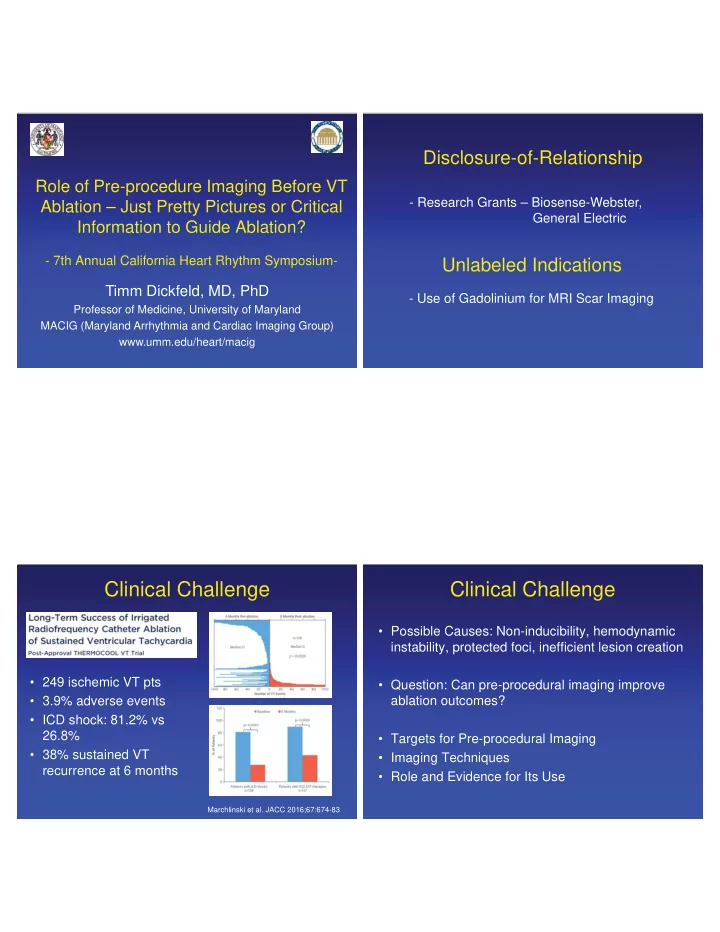
Disclosure-of-Relationship Role of Pre-procedure Imaging Before VT - Research Grants – Biosense-Webster, Ablation – Just Pretty Pictures or Critical General Electric Information to Guide Ablation? - 7th Annual California Heart Rhythm Symposium- Unlabeled Indications Timm Dickfeld, MD, PhD - Use of Gadolinium for MRI Scar Imaging Professor of Medicine, University of Maryland MACIG (Maryland Arrhythmia and Cardiac Imaging Group) www.umm.edu/heart/macig Clinical Challenge Clinical Challenge • Possible Causes: Non-inducibility, hemodynamic instability, protected foci, inefficient lesion creation • 249 ischemic VT pts • Question: Can pre-procedural imaging improve • 3.9% adverse events ablation outcomes? • ICD shock: 81.2% vs 26.8% • Targets for Pre-procedural Imaging • 38% sustained VT • Imaging Techniques recurrence at 6 months • Role and Evidence for Its Use Marchlinski et al. JACC 2016;67:674-83
Anatomic Evaluation Anatomic Evaluation - Cardica Anatomy - - Endocavitary Structures - • Underappreciated entity • 190 VT RFA • 24% ECS affecting case - 67% mapping (n=31) - 33% RF target (n=15) 8% of all cohort - 30% papillary muscle - 47% moderator band - 23% false tendon Chamber Anatomy Abbouezzeddine et al. JCE 2010;21:245; Doppalapudi et al. Circ Arrhythmia Electrophysiol. 2008;1:23 Good et a.. Heart Rhythm. 2008;:1530; Tian et al. Circulation 2008; 118:S690 Anatomic Evaluation Anatomic Evaluation - Myocardial Structures: VSD patch and Pledgets - - Epicardial Structures: CA, Epicardial Fat - • Coronary Arteries - 5-10mm safety distance; thermal injury with abrupt thrombosis or delayed VT PM SMC hypertrophy Semi-automatic CA Reconstruction • Epicardial Fat - Mapping: decreased �������������������� CT Integration VT termination post 11s - RF delivery not effective 56 yo pt, 6 weeks post with 3.5-7.3mm IMI with LV wall rupture Epi/Pericardial Fat and Fat Map • Phrenic Nerve and LV patch vanHulsvanTaxis et al. JACC:CV Im. 2 013 :6;42; Desjardins B et al. JACC. 2010;56: RF site co-localization 1320 ; d’Avila et al. Circulation 2004;109:2363; Saba M et al. Europace 2009;11:949
Scar Imaging Scar And MACE Anatomic Substrate of Reentrant VT %LGE/LV Inner Loop WMS% Isthmus Exit Blind Alley HR for MACE for % LGE/LV Outer Loop and WMS% • 195 likely CAD pts. (EF 54±14%) with 16m F/U • Threshold effect with HR of >7 with 1.4% LGE Adapted from Stevenson et al. Circulation. 1993;88:1647 Kwong R. et al. Circulation. 2006;113:2733 Critical Amount of Scar? Computed Tomography 4.3g myocardium = 1.4% LV mass
Computed Tomography Anatomic Evaluation - Calcification - Advances in Multi-detector CT - �� 256 slices; <0.4s gantry rotation Tissue HU Air 0 - submillimeter resolution; <1mSv radiation Bone 1000 Air -1000 • Anatomic Evaluation Ca++ >200 - Wall thickness, calcifications • Dynamic Evaluation - Wall motion, wall thickening • Perfusion Evaluation - First-pass hypoperfusion, delayed enhancement Calcification Comprehensive Scar Characterization; n=11 Anatomic Evaluation Anatomic Evaluation - Fatty Replacement - - Wall Thickness - Tissue HU Air 0 Bone 1000 Air -1000 2D-CT WT Segm. WT Ca++ >200 Contouring Analysis Fat -100 • Intramyocadial remoddelling with hypoattenuation • 22 post-MI patients undergoing VT ablation Segm. Volt. WT • 50% of VT circuits in close proximity to fat deposits Analysis Projection Sasaki et al. Heart Rhythm 2015;12:1508 Tian et al. Circ Arrhythm Electrophysiol 2010;3:496
Comparison of Anatomic/Dynamic Parameters between Dynamic Evaluation: Voltage-Defined Abnormal and Normal Segments Comparison with LV Voltage Map EDWT (mm) ESWT (mm) WT (%) WM (mm) 40 * 35.70 35 30 25 20 * * 15 10.88 10 8.12 * 5.77 5.69 5 2.68 0.96 0 P<0.05 * -2.48 -5 CT Image 17-Seg Analysis Voltage Map Normal Abnormal (WT) Normal segments (>1.5mV): 43 segments Abnormal segments (<1.5mV): 28 segments(5 scar, 3 BZ, 20 scar/BZ) Tian et al. Circ Arrhythm Electrophysiol 2010;3:496 Prediction of Abnormal Voltage Segments with Perfusion Anatomic and Dynamic Parameters - 1 st pass Hypoperfusion - • Regression Model: - ESWT and WT with Microvascular obstruction best prediction value - correctly classifies 82% segments Highly vascularized myocardium - AUC= 0.85 � 0.05 Relative vascular paucity Absolute and relative hypoperfusion Tian et al. Circ Arrhythm Electrophysiol 2010;3:496 Hearse et al. J Cardiovasc Res 2000;45:215; Nakano M et al. Circ Cardiovasc Imaging. 2011;4:597
Computed Tomography Correlation of Hypoperfusion and Voltage - Perfusion Characteristics: 1 st pass Hypoperfusion - • LV Scar Burden • 82% of successful RF • Perfusion CT: 33.3±8.5% sites in border zone Transmural Scar Endocardial Scar • Voltage <1.5mV: 37.4±11.4% • 18% in scar center • r=0.77, P=0.006 Tian et al. Circ Arrhythm Electrophysiol 2010;3:496 Delayed Contrast Enhancement First Pass and Late Enhancement Acute Acute Chronic Viable Myocardial Myocardial Myocardium Infarction Infarction Scar I I Na Na Na Na I I I I I I First Pass Na Na I K K Na I I “Black” Na I I K K K I Na I Na I I Na I I Na I K K I I Na I Late I K I Na K K I Na Na Enhancement Intact Collagen Ruptured “White” Cell Membranes Cell Membranes Matrix Tissue Volume Increased volume of Myocyte replacement, • 37 patients (16 acute, 21 chronic MI) predominantly intracellular distribution increased interstitial space/VoD (75%) Gerber BL. Circulation 2006; 113:823 Kim RJ, et al.: Lippincott Williams and Wilkins, 20
Computed Tomography Anatomic Evaluation - Perfusion Characteristics: Delayed Enhancement - - Comparison with EAM - 71 [59–124] cm2 54 [46–92] cm2 CT WT recon. EAM fusion (45 [42–61] cm2 52 [51–68] cm2 • 13 post-MI patients • CT wall thickness <5mm ~ endocardial <1.5mV Pre-contrast Post-contrast • LAVA: 87% within WT<5mm; rest within 23mm Komatsu Y et al. Circ Arrhythm Electrophysiol. 2013;6:342 Anatomic Evaluation -Wall Thickness in Non-Ischemic CM - Magnetic Resonance Imaging • Very limited data on NICM • 3/3 pts with wall thinning <5mm (1/3 with LGE) • 63 ± 21% overlap with <1.5mV Cochet H et al. JCE 2013:24;419
MRI: Near-Cellular SubstrateResolution Correlation: MRI and Voltage • LAD ligation Rat-infarct model • LGE ex-vivo 7T MRI • Voxel: 50x50x50 � m • MRI/histoloy correlation (R 2 =0.96) • Ability to detect clefts 2-4 myocytes thick DE MRI Voltage Map Schelbert et al. Circ Cardiovasc Imaging 2010;3;743 Correlation of Scar Transmurality and Voltage CMR: MRI Scar and Voltage Scar 7 r = 0.72 Bipolar Voltage [mV] 6 5 4 3 2 1 0 0 50 100 Scar Transmurality [%] 15 post-MI pts Wijnmaalen et al . Eur Heart J. 2011;32:104 Dickfeld et al. Circ Arrhythm Electrophysiol. 2011;4:172
MRI Scar and Voltage Mapping Mismatch: MRI Scar > Voltage Scar • Best voltage cut-off for MRI scar: - Bipolar voltage: 1.0-1.54mV - Unipolar voltage: 4.46-6.52mV Codreanu . JACC. 2008;52:839 Desjardins. Heart Rhythm 2009;6:644 Dickfeld . Circ Arrhythm Electrophysiol. 2011;4:172 A A • Comparison MRI and Voltage Scar Area: - MRI scar ~ <0.5mV scar area Nakahara . Heart Rhythm 2011;8:1060 - MRI scar ~ <1.5mV scar+border zone area B Desjardins. Heart Rhythm 2009;6:644; Dickfeld . Circ Arrhythm Electrophysiol. 2011;4:172 - MRI scar slightly larger than 1.5mV area Wijnmaalen . Eur Heart J. 2011;32:104 B • Significant Mismatch: 1/3 of patients • �������������������������������������������������� Codreanu . JACC. 2008;52:839 Wijnmaalen et al . Eur Heart J. 2011;32:104 Tian J et al. Heart Rhythm 2009; 6:825 Wijnmaalen et al. Eur Heart J. 2011;32:104 Dickfeld et al. Circ Arrhythm Electrophysiol. 2011;4:172; Mismatch: MRI Scar > Voltage Scar Mismatch: Voltage Scar > MRI Scar • Suboptimal Catheter Contact: - Frequently basal “pseudoscar” Codreanu A et al. JACC. 2008;52:839 Nakahara et al. Heart Rhythm 2011;8:1060 - Early registration algorithm (e.g. CartoSOUND) corrected 4.1±1.9% falsely low voltage points Dickfeld et al. Circ Arrhythm Electrophysiol. 2011;4:172 • Decreased MRI Sensitivity to detect patchy scar Nakahara et al. Heart Rhythm 2011;8:1060 • Limited Mapping Density: incorrect low voltage Endocardial layer of ~2mm normal myocardium masks extrapolation Desjardins et al. Heart Rhythm 2009;6:644 intramural scar (predominantly in septal location) Dickfeld et al. Circ Arrhythm Electrophysiol. 2011;4:172; Wijnmaalen et al.. Eur Heart J. 2011;32:104
MRI-Guided Ablation: Border Zone Image-Guided VT Ablation Pacemapping Guided by MRI Scar Pacemap Match Dickfeld et al. Circ Arrhythm Electrophysiol. 2011;4:172 MRI-Guided Ablation MRI-Guided Ablation: Abnormal Substrate - Successful Ablation Site Characteristics - 1 1 2 80-Sector Segmentation PM 2 2 PM 2 Surviving PM Substrate-Guided Mapping Pap. Muscle Match Reprojection of PM Site Transmurality Display Dickfeld et al. Circ Arrhythm Electrophysiol. 2011;4:172
Recommend










More recommend
Explore More Topics
Stay informed with curated content and fresh updates.