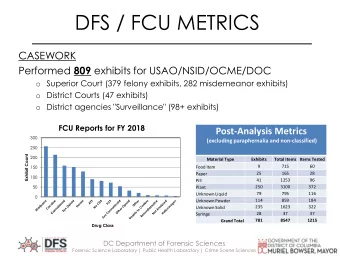
2/16/2014 AVOIDING THE CRASH: AVOIDING THE CRASH 1: DON’T INTUBATE , OPTIMIZE OPTIMIZE YOUR PRE, PERI, AND POST AIRWAY MANAGEMENT PRE-AIRWAY MANAGEMENT Robert J. Vissers MD Robert J. Vissers MD Chief, Emergency Medicine, Chief, Emergency Medicine, Quality Chair, Legacy Emanuel Medical Center Quality Chair, Legacy Emanuel Medical Center Adjunct Associate Professor, OHSU Adjunct Associate Professor, OHSU Portland, OR Portland, OR Objectives Adult Learner • Understand when not to intubate • Review the optimal airway management for the crashing patient in the ED • Prevent hypoxia and hypotension associated with intubation of the critically ill • Understand appropriate ventilator management to avoid patient deterioration • Be humble 1
2/16/2014 Adult Learner Intubating the critically ill • Focus on the Life Threat. A - B - C….D? “I need to intubate the • Differentiate shock state - will intubation patient …but I know make it better or worse? he’ll crash when I do.” • Optimize physiology first • It’s a team sport Approach to the Approach to the Decision to Decision to Emergency Airway Emergency Airway intubate intubate Near death? Near death? TIME TIME Unresponsive? Unresponsive? Difficult ANATOMY Difficult ANATOMY Airway? Airway? RSI Rapid PHYSIOLOGY PHYSIOLOGY Post Intubation Sequence Management Intubation Adapted from: Walls RM, Ed. The Manual of Emergency Airway Management Philadelphia, Lippincott, 2000. Adapted from: Walls RM, Ed. The Manual of Emergency Airway Management Philadelphia, Lippincott, 2000. 2
2/16/2014 Approach to the Decision to Intubating the critically ill Emergency Airway intubate • Planning is critical – no margin for error Near death? • Assess and plan for difficulty TIME Unresponsive? • Optimize physiology – focus on prevention of hypoxia and hypotension Difficult ANATOMY • Airway may come second Airway? • Use a checklist – inform the team RSI PHYSIOLOGY Post Intubation Management Adapted from: Walls RM, Ed. The Manual of Emergency Airway Management Philadelphia, Lippincott, 2000. Cardiac arrest: The rise of “C” Keys to success: Teamwork “C” Circulation precedes Teamwork • Time out Airway and Breathing • Share the plan • Leadership • Help 3
2/16/2014 Cardiac arrest: Don’t pause for airway Cardiac arrest: Compressions First Key to success: Key to success: • High quality, uninterrupted chest compressions • High quality, uninterrupted chest compressions • Airway can wait • Airway can wait • Passive ventilation may be superior to positive • Passive ventilation pressure ventilation • 30:2 compression/breath • Consider supraglottic airway without interruption • Supraglottic airway: LMA, King-LT, combitube Bobrow BJ, et al. Passive oxygen insufflation of oxygen superior to BVM for witnessed VF arrest. Ann Emerg Med, 2009. Cardiac arrest: Capnography Cardiac arrest: Capnography • Confirm tube placement • Confirm tube placement • Assess quality of CPR • Assess quality of CPR • Identify ROSC without pulse check • Identify ROSC without pulse check • Predict outcome • Predict outcome • Highly reliable (Class 1 evidence) • Ideally ETCO2 of 20-25 mmHg • May be low after prolonged arrest • Correlates with quality of compressions, CPP • Cannot identify right main stem 4
2/16/2014 Cardiac arrest: Capnography Cardiac arrest: Capnography • Confirm tube placement • Confirm tube placement • Assess quality of CPR • Assess quality of CPR • Identify ROSC without pulse check • Identify ROSC without pulse check • Predict outcome • Predict outcome • Sudden rise in ETCO2 suggests ROSC • Persistent ETCO2 < 10 ROSC is unlikely • More sensitive then manual pulse checks • <10 after 20 minutes, zero ROSC in studies Mayer SA, et al. Efficacy and safety of factor VII for acute ICH. NEJM, 2008. Adult Learner Airway the shock patient • Focus on the Life Threat. A - B - C….D? • Primary goal: avoid exacerbation of hypoperfusion • Differentiate shock state - will intubation • Need to differentiate shock state make it better or worse? • Consider before intubation: • Optimize physiology first • Assessment of volume status • It’s a team sport • IVFs as pretreatment before intubation • Vasopressor before intubation • A vs C: hemodynamic compromise vs hypoxia 5
2/16/2014 CP/SOB/hypotensive • 48 y.o. female hx of breast cancer • Pleuritic chest pain, dyspnea, anxiety • BP 92/58, P 132, RR 28, O2 sat 95% • Lungs clear, JVD • CXR borderline cardiomegaly Massive PE vs Pericardial Tamponade Massive PE vs Pericardial Tamponade PE vs Pericardal tamponade • Ultrasound helpful • Effusion in tamponade • Both present similar way • Treatment very different • Need to distinguish before intubation 6
2/16/2014 Massive PE vs Pericardial Tamponade Massive PE vs Pericardial Tamponade • Ultrasound helpful • Pulmonary Embolism • RV septal bulging in PE • Preload sensitive, IVF may worsen RV overload • Pressors for hypotension • Intubation may help – reduced preload, O2 • Lytics if unstable • Pericardial tamponade • Need preload – IVF helpful • Intubation may worsen hypotension • Pericardiocentesis Adult Learner Septic shock • Focus on the Life Threat. A - B - C….D? • 32 yo male, hx of paraplegia from GSW, chronic decubitus ulcers, cocaine and non-compliance • Differentiate shock state - will intubation • BP 92/58, P 132, RR 28, O2 98% RA make it better or worse? • Agitated, delirium, horrible deep buttock • Optimize physiology first ulcerations to bone, maggots, no crepitus • It’s a team sport 7
2/16/2014 Intubating the shock patient Adult Learner • Focus on the Life Threat. A - B - C….D? Optimize physiology - Perfusion • Almost all patients need volume • Differentiate shock state - will intubation • 40mL/Kg in kids make it better or worse? • 1-2 liters in adults • Optimize physiology first • May delay intubation if • It’s a team sport hypotensive, or hypovolemic and O2 OK – perfusion priority • Fluids/pressors Pediatric FB Management • 5 yo girl, choked on peanuts last night • BLS: Infant: 5 back blows/5 chest thrusts • Unable to sleep, trouble breathing • Looks tired, resp distress, tripod • Foreign objects can be lodged in the upper or lower airway, or esophagus. • Stable partial obstruction – leave alone but prepare for the worst 8
2/16/2014 Management ED Management • Laryngoscopy and • BLS: Child: 5 abdominal thrusts removal with pediatric Magill forceps • 1/3 of pediatric FBs are at cords or above ED Management Adult Learner • Focus on the Life Threat. A - B - C….D? • What if it is a tracheal • Differentiate shock state - will intubation obstruction? make it better or worse? • Abdominal thrusts • Optimize physiology first • May need to push into • It’s a team sport right mainstem 9
2/16/2014 Thankyou! 10
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries