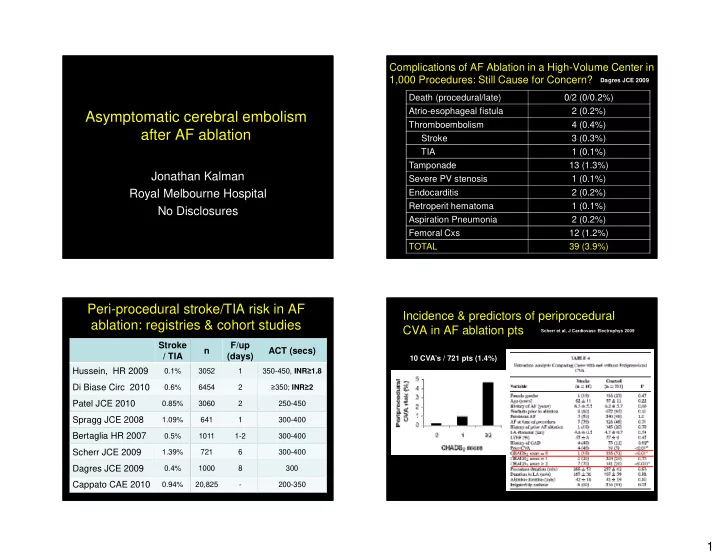
Complications of AF Ablation in a High-Volume Center in 1,000 Procedures: Still Cause for Concern? Dagres JCE 2009 Death (procedural/late) 0/2 (0/0.2%) Atrio-esophageal fistula 2 (0.2%) Asymptomatic cerebral embolism Thromboembolism 4 (0.4%) after AF ablation Stroke 3 (0.3%) TIA 1 (0.1%) Tamponade 13 (1.3%) Jonathan Kalman Severe PV stenosis 1 (0.1%) Royal Melbourne Hospital Endocarditis 2 (0.2%) Retroperit hematoma 1 (0.1%) No Disclosures Aspiration Pneumonia 2 (0.2%) Femoral Cxs 12 (1.2%) TOTAL 39 (3.9%) Peri-procedural stroke/TIA risk in AF Incidence & predictors of periprocedural ablation: registries & cohort studies CVA in AF ablation pts Scherr et al, J Cardiovasc Electrophys 2009 Stroke F/up n ACT (secs) / TIA (days) 10 CVA’s / 721 pts (1.4%) Hussein, HR 2009 0.1% 3052 1 350-450, INR ≥ 1.8 Di Biase Circ 2010 0.6% 6454 2 ≥ 350; INR ≥ 2 Patel JCE 2010 0.85% 3060 2 250-450 Spragg JCE 2008 1.09% 641 1 300-400 Bertaglia HR 2007 0.5% 1011 1-2 300-400 Scherr JCE 2009 1.39% 721 6 300-400 Dagres JCE 2009 0.4% 1000 8 300 Cappato CAE 2010 0.94% 20,825 - 200-350 1
Atrial “stunning” immediately post Potential mechanisms underlying RF flutter reversion thromboembolism in AF ablation procedures Sparks, Kalman JACC 1999 Chronic Atrial Flutter Sinus Rhythm • AF reversion: atrial “stunning” 40 cm/s 0 cm/s • Multiple intra-LA catheters/sheaths • Char formation • Endothelial disruption LA LASEC • Activation of coagulation factors LV LV Increased anticoagulation intensity reduces thrombus risk during AF ablation LA Thrombus Ren et al, J Cardiovasc electrophysiol 2005 During AF RFA: Incidence of ICE detected mobile thrombus ICE Imaging (on sheath/catheter after T/septal) Ren et al, JACC 2004 ACT ACT >300 p 250-300 • ACT >250 All pts • LA thrombus in 24/232 pts (10.3%). 11.2% 2.8% <0.05 (n=511) • Thrombi 12.9 X 2.2 mm (width) • Attached to sheath or mapping catheter. Pts with • Thrombi (27 of 30, 90%) aspirated into sheath 44.9% 4.6% <0.0001 SEC (n=179) • No clinical embolic events. • SEC, best predictor on multivariate analysis 2
Phased-Array ICE monitoring during PVI in pts Phased-Array ICE monitoring during PVI in pts with AF: Impact on outcome & complications with AF: Reduction of embolic events Marrouche et al. Circulation 2003: 107: 2710 Marrouche et al. Circulation 2003: 107: 2710 Type 2 bubbles Type 1 bubbles Dense Microbubbles Scattered Microbubble Imminent impedance rise Early Tissue Overheating → Power reduced by 5 watts → RF turned off Calkins HR 2012 Calkins HR 2012 2012 HRS/EHRA/ECAS Expert Consensus 2012 HRS/EHRA/ECAS Expert Consensus Statement on AF Ablation Statement on AF Ablation Anticoagulation mgt pre ablation Anticoagulation mgt during ablation • If >48 hrs AF at time of ablation follow DCR guidelines • Heparin prior to or immediately following trans-septal – ie. TEE or 3 weeks prior anticoagulation puncture to achieve and maintain an ACT of 300-400 secs. • TEE in pts in SR may be considered but is not • Intravenous heparin to ACT 300-400 secs should be given mandatory even if pt on warfarin • Catheter ablation of AF during therapeutic warfarin • Heparinised saline irrigation of long sheaths anticoagulation should be considered 3
Cerebral Diffusion-Weighted MRI: Monitoring AF Ablation: A Cause of Silent Embolism? Thrombogenicity of LA Ablation Lickfett JCE 2006 Gaita, Circ 2010 • Cerebral MRI pre & post AF ablation (irrigated tip) • 2/20 pts (10%) with new MRI lesion Open irrigated RF for AF 232 procedures • No neurological sequelae PVI 47% 1 day post-AF RFA 3 mths post-AF RFA PVI + linear 37% PVI + linear + CFAE 16% Procedure duration 182 mins RF time 46 mins Mean ACT 281 secs ACT<250; 250-300; >300 18%; 57%; 25% SR; SR with RFA; SR with DCR 48%; 25%; 27% Relation of DCR and ACT to incidence AF Ablation: A Cause of Silent Embolism? of silent emboli Gaita, Circ 2010 Gaita, Circ 2010 • 232 consecutive pts pre & post AF ablation MRI DCR RF reversion SR • New embolic lesions 33 pts (14%) throughout Embolic rate 26% 14% 9% • Lesion number: 25 pts- 1 ; 3 pts - 2; 5 pts – 3 • Lesion size: 3 to 35 mm diameter. ACT <250 ACT >250 • No clinical parameters predictive Silent Emboli incidence 17% 9% – age, HT, DM, prior stroke, AF type, pre-RF antithrombotics Emboli DCR pts 29% 21% • Procedural parameters were predictive Emboli No DCR pts 13% 4% – ACT No silent emboli observed in 65 PeAF pts – DCR (Rel Risk 2.75; p=0.009) undergoing DCR alone 4
Delaying DCR for 4-weeks anticoagulation MEDAFI-Trial (Micro-emboli during AF RFA) Neumann, Europace 2011 in persistent AF after ablation to reduce silent Cerebral lesion No cerebral lesion cerebral embolism: a single-center pilot study 7 pts 82 pts 7.9% Pianelli, Gaita. J Cardiovasc Med 2011 Delayed DCR if Historical controls: 20 variables in AF (95 pts) DCR if in AF (95 pts) New MRI lesions 6% 16% (p=0.03) New lesions DCR grp 2/15 (13%) 11/29 (38%) 4 delayed DCR All seven patients had PAF, low CHADS score, and No. of pts involved 29 Early DCR (11 late spont SR) no pre-existing cerebral MRI abnormalities ACT (mean secs) 297±56 268±28 Persistent AF 28% 38% Asymptomatic Emboli After PVI: Incidence of silent cerebral thromboembolism after AF ablation by technology used Comparison of Different AF Ablation Gaita, JCE 2011 Technologies in a Multicenter Study 108 pts undergoing AF ablation p=0.001 Herrera-Siklody, JACC 2012 Non-randomized p=0.002 p=0.5 Irrigated RF Cryoballoon PVAC 40 38.9 (n=27) (n=23) (n=24) 30 Silent 2 (7.4%) 1 (4.3%) 9 (37.5%) % Non-randomized emboli 20 Emboli/pt 1 1 2.7 Embolus 6 4 6.0 (4.5-8.5) 10 size (mm) 8.3 5.6 ACT>300 secs; PVI only PVAC Irrigation cryo 5
Trans-cranial Doppler to Measure Cerebral New silent MRI lesions after AF ablation: Microembolic Signals During PV Isolation: Incidence by ablation modality Comparison of 3 RF Techniques Sauren, JCE 2009 n Age ACT RF Cryo PVAC Solid tip Irrigated RF Cryoballoon Schrickel, EPace 2010 53 53 >250 11.3% - - 4500 p=0.001 4000 250- Gaita, Circ 2010 232 58 14.2% - - 3500 300 p=0.001 3000 Neumann EPace 2011 89 46-63 >300 6.8% 8.9% - 2500 2000 Schwarz HR 2011 21 54 >300 9.5% - - 1500 p=0.027 1000 H Siklody JACC 2011 500 74 61 >300 7.4% 4.3% 37.5% 0 MES total Ablation period Manipulation Gaita JCE 2011 108 56 >300 8.3% 5.6% 38.9% period Post-RF asymptomatic cerebral lesions: Post-RF asymptomatic cerebral lesions: Long-term follow-up using MRI imaging Long-term follow-up using MRI imaging Deneke, Heart Rhythm 2011 MRI D1 post ablation Deneke, Heart Rhythm 2011 5 small, 1 large lesion • 86 pts having AF ablation • 84% with PVAC • 33/86 pts (38%) had new cerebral lesions – 30/33 (91% PVAC) • 14/33 (42%) had repeat late MRI (2 wks-1yr) MRI 2 mths post ablation 5 small lesions no longer visible • These 14 pts – 50 lesions @ D1 (3.6 lesions/pt) – 3 lesions @ late repeat MRI 6
Cardiac surgery incidence of new silent MRI lesions Post-RF asymptomatic cerebral lesions: New Lesion size n Surgery lesions Deneke, Heart Rhythm 2011 Bendszus, 2002 35 26% On pump CABG Restreppo, 2002 13 31% On pump CABG Knipp 2004 29 45% On pump CABG Djaiani, 2004 50 16% On pump CABG Stolz, 2004 37 38% AVR Knipp, 2005 30 47% Valve Friday, 2005 16 31% Off pump CABG Floyd, 2006 34 18% Valve & CABG Cook, 2006 50 32% Valve & CABG Barber, 2008 40 43% Valve & CABG Gerriets, 2010 86 15% On pump CABG TOTAL 446 29% Neurocognitive abnormalities and micro- AF is independently associated with senile, emboli in other cardiac procedures vascular, & Alzheimer’s dementia Bunch, Heart Rhythm 2010 • CAB Surgery Newman. NEJM 2001;344:395-402 • 37,025 pts mean age 60.6 yrs – 40% POCD > 5yrs post surgery Bladin. Stroke 1998;29:2367-70 • 5 yr follow-up • Valve surgery Pugsley. Stroke 1994;25:1393-99 – 27% AF – 50-97% incidence micro-emboli with mechanical valve – 4.1% Dementia – 23% POCD<1 mth post surgery • Dementia risk assoc d with: • Left heart catheterisation – Age, HT, CAD, CHF, Prior CVA – Asymptomatic microembolism in >50% pts • AF independently assoc d with Dementia – 16.7% POCD 24 hours post procedure 7
AF is independently associated with AF is independently assocd with senile, vascular, & Alzheimer’s dementia senile, vascular, & Alzheimer’s dementia Bunch, HR 2010 Bunch, Heart Rhythm 2010 Highest rel risk in younger age group AF in stroke-free pts: associated with MEDAFI-Trial (Micro-emboli during AF RFA) memory impairment & hippocampal atrophy Incidence of pre-existing MRI lesions Knecht, European Ht J. 2008 Neumann, Europace 2011 RF (n=44) Cryo (n=45) P Mean performance - Learning & Memory Hippocampal volume Pre-existing MRI 15.9% 8.9% ns lesions Age 58 56 ns PAF 61% 100% <0.001 CHADS 2 ≥ 2 11% 2% ns CHF 11% 2% ns HT 59% 51% ns Warfarin 59% 42% ns 8
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries