Application of QSP modeling to possible pharmacological targets in - PowerPoint PPT Presentation
Application of QSP modeling to possible pharmacological targets in Alzheimers disease Oleg Demin, Tatiana Karelina, Sergey Belykh, Oleg Demin Jr Institute for Systems Biology SPb, Moscow, Russia Timothy Nicholas, Hugh A. Barton, Yasong Lu,
Application of QSP modeling to possible pharmacological targets in Alzheimer’s disease Oleg Demin, Tatiana Karelina, Sergey Belykh, Oleg Demin Jr Institute for Systems Biology SPb, Moscow, Russia Timothy Nicholas, Hugh A. Barton, Yasong Lu, Sridhar Duvvuri Pfizer Global Research and Development, Groton, CT USA Loughborough, September 7, 2012
Outline • When and How Quantitative Systems Pharmacology (QSP) Modeling can contribute to discovery and development of new drugs • Application of QSP modeling to possible pharmacological targets in Alzheimer’s disease
Systems Pharmacology Modeling: definition and comparison with other modeling techniques • Systems Pharmacology (SP) Modelling is a technique for quantitative dynamic description of regulatory mechanisms of disease development/progression and mechanisms of drug action at intracellular/tissue/organism levels. • SP Modelling combines disease-specific description of intracellular pathways, cell dynamics, drug pharmacokinetics, tissue cross-talks and allows to express intracellular effects of the drug in terms of clinically measured biomarkers and end-points. Systems biology Systems pharmacology PK/PD modelling Typically intracellular or molecular Conceptually developed at the scale of Typically developed at the organism level interest , but is usually at a tissue/organ scale reflecting typical data collected scale to provide compatibility with PKPD models Highly granular typically all network Intermediate in granularity ; typically Low granularity ; typically no further intermediates and their mechanistic considers key network intermediates; may layer of complexity than observation linkage are captured. (network-level) contain mechanistic and empiric (input/output-type model; target relationships between intermediates level) (pathway level) Assumption rich , typically need Assumption-rich ; may need experimental in Low in assumptions ; no further in experimental data to calibrate vitro data to calibrate vitro data required to calibrate Agoram B, Demin O; Drug Discov Today, 2011 Dec;16(23-24):1031-6.
How different types of modeling contribute to drug R&D Agoram BM, Demin O; Drug Discov Today , 2011 Dec;16(23-24):1031-6.
How systems pharmacology modelling could be implemented in drug discovery projects. • From an initial evaluation of the literature and input from disease biology experts an initial mathematical model can be constructed (Iteration 1). • The predictions of this model are subject to feedback from a wider expert panel and subsequently this iteration (Iteration 2) is used to identify critical assumptions and testable hypotheses. At this stage the determination of key system parameters such as target molecule concentrations (biomeasures) are likely to be critical. • An iteration of the model is then produced that is consistent with these data (Iteration 3). This model can be used to predict clinical outcome and contribute to trial design eg initial dose prediction. Finally, the actual result can be compared to predictions and the conclusions Benson N, Cucurull-Sanchez L, Demin O, Smirnov S, van der Graaf P.; incorporated in subsequent Adv Exp Med Biol ., 2012;736:607-15 rounds
Systems Pharmacology Modelling is mainly focused on… • Build an understanding of the systems of interest, integrating available biological data • Hence, to identify the right target(s), the right modality, the dose and to evaluate critical project risks • Answer defined & specific but complex questions requiring M&S to draw conclusions • To help progress projects more rapidly & cost effectively to market to.. • Kill highest risk projects early & focus on most tractable • Identify hypotheses that can be tested at an early stage • Progress ideas where no animal model of disease or pharmacology • Identify optimal biomarkers and precision medicine strategies
Systems Pharmacology Modelling is mainly focused on… • Build an understanding of the systems of interest, integrating available biological data • Hence, to identify the right target(s), the right modality, the dose and to evaluate critical project risks • Answer defined & specific but complex questions requiring M&S to draw conclusions • To help progress projects more rapidly & cost effectively to market to.. • Kill highest risk projects early & focus on most tractable • Identify hypotheses that can be tested at an early stage • Progress ideas where no animal model of disease or pharmacology • Identify optimal biomarkers and precision medicine strategies
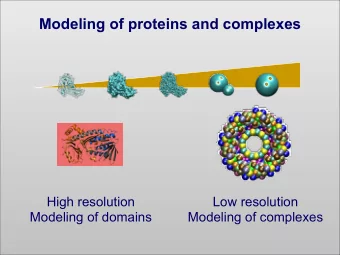
Application of QSP modeling to possible pharmacological targets in Alzheimer’s disease • Alzheimer's disease ( AD ) is the most common form of dementia. There is no cure for the disease. • The cause and progression of AD are not well understood. Research indicates that the disease is associated with senile plaques (extracellular deposits of amyloid ) and neurofibrillary tangles (intracellular aggregates of hyperphosphorylated tau protein ) in the brain. • Abeta cascade hypothesis: AD begins with the formation of Abeta, the oligomerization, and then the formation of insoluble plaques. ‘Toxic’ species of Abeta leads to neurodegeneration (Hardy 1992, 2002, 2009). This toxic species are related to either soluble monomeric or soluble oligomeric Abeta . Abeta plaques are in equilibrium with the soluble ‘toxic’ species of Abeta. • Removal of the plaque would result in absence of a source for a ‘toxic’ species of Abeta.
Application of QSP modeling to possible pharmacological targets in Alzheimer’s disease • Removal of the plaque would result in absence of a source for a ‘toxic’ species of Abeta. • The effect of Abeta production/clearance modulators have been tested clinically with no observed cognitive benefit . • A possible reasons are - the potency of the compounds tested was not sufficient to have an effect - the exposure of the compounds was not sufficient to test the potency in the clinical trial for the duration necessary. QUESTION: How to estimate optimal potency/exposure of the modulators for Abeta production/clearance? ANSWER: To develop QSP model of Abeta aggregation in human
Types of the data available (1) in vivo data obtained by post-mortem autopsy for healthy subjects and for AD patients (Ab40, Ab42: soluble and unsoluble measured in nM) (2) Abeta production/clearance ration measured for AD patients in vivo (3) Positron Emission Tomography (PET) data measured in vivo for for healthy subjects and for AD patients
Positron Emission Tomography Positron Emission Tomography (PET) provides in vivo evidence of the local accumulation of a specific radioligand and allows to estimate quantitative features of the binding sites (their number and affinity) for this radioligand. In the case of Alzheimer Disease there is radioligand PIB that could bind with Amyloid Fibrils (with some motifs on fibril). Thus, this method allows to estimate quantity of monomers in all fibrils in vivo. Standardized Uptake Value [SUV] and Distribution Volume [DV] of radioligand for particular region of the brain or Ratio of Standardized Uptake Values [ SUVR ] and Ratio of Distribution Volumes [ DVR ] of 2 regions in the brain are the main parameters that represented the results of PET. How to understand/express PET data in terms of Abeta aggregation mechanisms?
Application of QSP modeling to possible pharmacological targets in Alzheimer’s disease Aims : • to develop model of Abeta aggregation in vivo for human and to verify it against postmortem data • to describe PET data in terms of variables of model developed; to validate the model against available PET data measured for both healthy subjects and AD patients • to apply the model to predict/understand effects of pharmacological interventions directed toward - inhibition of Abeta synthesis (25%, 50% or 100%) - increase in Abeta clearance (2-fold or 10-fold) initiated at 40, 50 or 65 years of age, were performed.
Main processes of Ab aggregation and oligomerization Our model is based on 3 different models from P i – Ab forms: [ Science. 2009 Dec 11;326(5959):1533-7 ](this P 1 – monomer model includes only fibrils), [ Nucl Med Biol. 2005 P 2 …P n-1 – different oligomers May;32(4):337-51 ](this model includes monomers P n – nucleus (= fibril with i=n) and fibrils, also in this model PET is described) and P j , where j = from (n+1) to infinity – fibrils [ Biophys J. 2007 May 15;92(10):3448-58 ](this model includes oligomerization and fibrillation). Oligomerization: Assumptions that we used to create the model: P 1 P 1 P 1 P 1 P 2 P 3 ……… P n-1 1. Only monomer could bind to other forms. P 1 Nucleation: 2. Parameters (both forward and reverse) for P n or P n-1 P n n*P 1 oligomerization and fibrillation are different. Fibrillation: P 1 P 1 3. The reverse fibrillation (depolymerization) P n P n+1 P n+2 ……… infinity and fibrils breakage have equal rate constants. Fibrils breakage: Fibril + Fibril 4. All reactions are described by mass action P j Fibril + Oligomer law. Oligomer + Oligomer
Recommend







More recommend
Explore More Topics
Stay informed with curated content and fresh updates.