
Alveolar echinococcosis: clinical case pres- entation Gabija Baguyt - PDF document
RADIOLOGY UPDATE VOL. 4 (7) ISSN 2424-5755 Alveolar echinococcosis: clinical case pres- entation Gabija Baguyt 1 , Paulina Tekoriut 1 , Diana Barkauskien 2 1 Lithuanian University of Health Sciences, Academy of Medicine, Faculty of
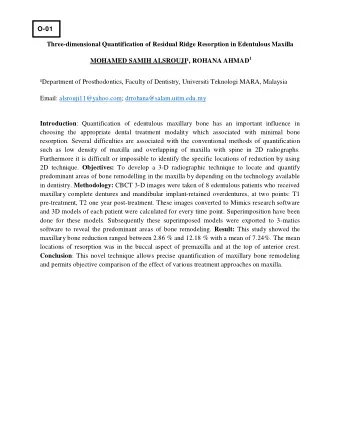
RADIOLOGY UPDATE VOL. 4 (7) ISSN 2424-5755 Alveolar echinococcosis: clinical case pres- entation Gabija Bagužytė 1 , Paulina Tekoriutė 1 , Diana Barkauskienė 2 1 Lithuanian University of Health Sciences, Academy of Medicine, Faculty of Medicine, Kaunas, Lithuania 2 Department of Pulmonology, Lithuanian University of Health Sciences, Kaunas, Lithuania ABSTRACT Echinococcosis is a parasitic disease caused by Echinococcus species. Tapeworm Echinococcus multilocularis causes alveolar echinococcosis (AE) which is a signifjcant worldwide public health problem with potential life-threatening outcomes. We present a case report of advanced AE with lesions in liver and dissemination to vena cava inferior and lungs. Keywords: echinococcus multilocularis, Alveolar echinococcosis, Malignant parasite, Mimicking cancer. INTRODUCTION difguse 13-17 mm diameter high-density forma- tions on both sides in the lungs. Tie patient was Echinococcosis is a zoonosis caused by a tape- referred to a pulmonologist for a further exami- worm species belonging to the genus Echino- nation suspecting a malignant process. coccus, family Taeniidae (1, 2). In humans, E. Second X-ray scan was performed showing mul- granulosus occurs as cystic echinococcosis, E. tiple high-density various sizes with the largest multilocularis causes alveolar echinococcosis measuring approximately 15 mm mass lesions (AE), and E. vogeli and E. oligarthrus as poly- with clear boundaries, mostly in the periphery cystic echinococcosis (3). E. multilocularis tape- of the lungs (Figure – 1). Radiological fjndings worm is endemic in many regions of the world, are to be difgerentiated with primary cancer and but parts of the Northern hemisphere, such as metastasis. North America, China, central and eastern Eu- Tie patient claimed to be allergic to iodine and rope and the Baltic states, are the most concern- therefore, was hospitalized for computed tomog- ing (4, 5, 6). In Lithuania alone between 1997 and raphy (CT) scan. On the day of admission, her 2013, a total of 179 AE cases have been reported vitals were normal, vesicular breathing and no (7). Diagnosing this disease is complicated due crackles were present. A consensus was made to to extended incubation time, various clinical perform a CT scan for suspected lung tumour manifestations and mimicking of difgerential di- and spreading during a pulmonologists Concili- agnoses (8). We report a case of advanced AE, um. Tie patient was treated with dexamethasone which is a rare infection and may even have fatal and clemastine according to the protocol against consequences. Our purpose is to raise awareness iodine allergy. of diagnosing this condition among various phy- Contrast-enhanced chest and abdominal CT re- sicians. vealed multiple polisegmental heterogenic-den- sity various size mass lesions with a policycle CASE REPORT outline situated along the vessels mostly in the periphery of both lungs, some with mild en- A 59-year-old woman referred by a general prac- titioner to the pulmonology department pre- hancement. Tie most prominent lesion is meas- uring approximately 16 x 11 mm in the right fjrst sented to our hospital with complaints of cough- ing up phlegm and blood, and weight loss. lung segment (Figure – 2, 3). CT also showed During a preventative health examination, a a heterogenic mild enhancement lesion with a policycle outline, cystic components and calci- front chest X-ray was performed, and it revealed 25
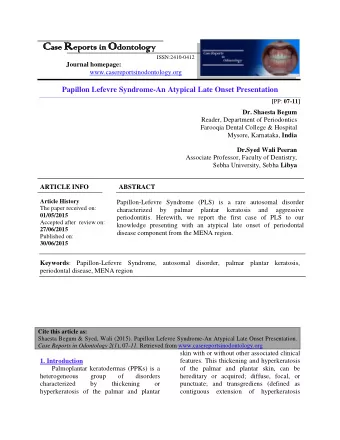
JOURNAL AVAILABLE AT RADIOLOGYUPDATE.ORG fjcations measuring approximately 12 x 82 x 78 mm, in the lefu lobe of the liver (Figure - 4). Vena cava inferior (up to right atrium level) and the vault of the diaphragm were also infjltrated. A few merging similar structures pathologic nodes measuring approximately 28 x 15 mm and nodules situated along the oesophagus with the largest measuring approximately 12 x 12 mm were present between the lefu lobe of the liver and the lesser curvature of stomach within the lefu heart ventricle. With these fjndings, hepatic echinococcosis with invading to vena cava infe- rior and hematogenous lung dissemination were suspected radiologically. Initial laboratory tests showed haemoglobin lev- Figure 2. Chest CT, coronal view - multiple polisegmen- el 147 g/l, white blood cells count 12,3 x 109/l, tal heterogenic-density mass lesions situated along the vessels mostly in the periphery of both lungs. eosinophils 0,0 x 109/l, platelet count 268 x 109/l. C – reactive protein, creatinine, urea, alanine and aspartate aminotransferase, and electrolytes were normal. In addition, the patient was pos- itive for the presence of IgG antibodies against Echinococcus spp. 74,2 g/l. Based on the clinical symptoms, imaging exam- inations, and serology test, Echinococcus multi- locularis infection was diagnosed. Albendazole treatment in 400 mg two daily doses was started, and the patient was referred to an infectologist for an immediate consultation. Figure 3. Chest CT, axial view - multiple mass lesions with a policycle outline mostly in the periphery of both lungs. Figure 1. Plain chest X-ray – multiple various size mass lesions in the periphery of both lungs Figure 4. Tioraco-abdominal CT, coronal view - a heter- ogenic mild enhancement lesion, cystic components and calcifjcations in the lefu lobe of the liver 26
Recommend



More recommend
Explore More Topics
Stay informed with curated content and fresh updates.