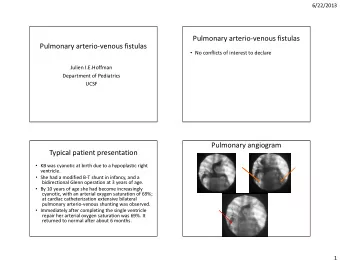
A CASE PRESENTATION BENEFITS OF PULMONARY REHABILITATION B Y E S T H E R S . A J J A R A P U , M . D , M . B A “ B U T Y O U B E S T R O N G A N D D O N O T L O S E C O U R A G E , F O R T H E R E I S R E W A R D F O R Y O U R W O R K ” .
DISCLOSURE I have no no actua ual or po potential conf nflict of int nterest i in n relation t to this pres esentation This present ntation n is s strictly y for inf nformationa onal/educ ucationa onal purpose onl nly Patient cons nsented to sharing h his i information
SPECTRUM OF COPD DIAGRAM COURTESY OF MEDSCAPE
GOLD CLASSIFICATION OF COPD FEV FEV 1 /FVC FEV FEV 1 1 FEV 1 >80% I I - Mild CO COPD D < < 0. 0.70 70 >80% p pre redicted FEV 1 50% II II - Moderate CO COPD D < < 0. 0.70 70 50% -79% p predicted FEV 1 30% III III - Severe C COPD < 0. < 0.70 70 30% - 49% 49% FEV 1 <30% IV - Very S y Severe C COPD < < 0. 0.70 70 <30% OR OR <50% <50% with s signs o of f chroni onic r respirator ory failur ure
DEFINITION OF PR • “…a m multid idisciplinary progr gram m of c care for patients w with chr hronic r respiratory impairment t that i is i individually lly tailored and designed to optimi mize ze eac each p pat atien ent’s ph physical and nd s social pe performance a and nd a aut utonomy.” ( (NICE CE) • "c "compr prehensive i int ntervention based on n a thorough pa patient a assessment followed by patient nt-tailored ed therapies es t that i include, , but are not l limi mited ed to, exercise training, g, education, , and b behavior c change, , designed t to o improve the p phys ysical a and ps psychological cond ndition o of pe peopl ple with c chronic r respiratory disease a and nd to pr promote the l long ng-term a adherence t to o health-enh nhanc ncing ng b behavior ors“ ( (ATS) E ERS) Amer Am erican an As Association of Car ardiovas ascular ar an and Pu Pulmonar ary Reh ehab abilitation ( AACVPR VPR) American A n Association n for R Respi piratory Ca Care ( AARC) Centers f for Medi dicare and d Me Medi dicaid Se Services ( (CMS) S)
GOALS-PR Reduced respiratory symptoms and complications Improved exercise performance Maintenance of emotional well being Reduced read eadmissions an and hospital alizations
CONTRAINDICATIONS--PR Contraind aindic icat atio ions ns to p pulmonar nary r rehabil ilitat atio ion n inc nclude c cond nditions th that w woul uld pl place t the e pa patien ent a at increased r risk k during e exer ercise or p present obst stacles t s to participation Co Coronary ar artery dise disease intra ractable le C CHF severe re arthrit itis, is, n neurologic ic i impair airment, c cognit itive o or psychoso social ial d disorde ders
INDIVIDUAL TREATMENT PLAN (ITP) The ITP mus ust f focus us o on n 4 domains : Ex Exerc rcise Nut utrition Educ ucation Psy sycho-so social well l being of of the patient
HISTORY OF ILLNESS-4/2015 63 year o old Ca Cauc ucasian m male w with mul ultiple pul pulmonary cond nditions was r referred t to pul pulmonary rehab b by his pul pulmonologist 4 4/2015 Work h history: Wor orked in t the mi mines in u underground m mining Worked f for 20 years as a cont ntinuous m mine ner ope perator and nd an n electrician Disable led i in 1991
PERTINENT MEDICAL HISTORY Obstructive Sleep Apnea w w/use of of C-PAP (1 (14 cm 4 cm H2O) 2O) Int nterstitial l lung ung d disease COPD PD Obe besit ity Co Compl plicated Pne neum umoconiosis/Pulmonary fibrosis Hypertens nsion, n, Anxiety, C Chroni onic P Pain
SURGICAL HISTORY Lum umbar f fus usion-2002 2002 Ca Carpa pal Tun unnel sur urgery -2004 2004 Prostatectomy d due ue to pr prostate c canc ncer-2005 2005 Socia ial l History: For orme mer S Smok moker- Smoked i intermittently for 15 years, ½ ½ to 1ppd ppd
MEDICATIONS-RESPIRATORY Spiriva— (tio iotropium br bromid ide-anticholinergic-prom omoting m m3 smoo mooth m muscle relaxation on Symbic bicort—QD(budesonide/formotero rol fumarate d dihy hydrate-inh nhaled c corticos osteroi oid + + long g ac acting g b2 ago agonist) ProAir—PRN(alb lbuterol) l) Ipratro ropium-albu buterol nebs bs (antic icholin inergic ic-bronchodilation) Oral t theop ophylline ne 300m 300mg –BI BID-- --bro ronchodilators O2 O2—cont ontinuous nuous at 2L—via ia NC
PULMONARY REHAB--RESULTS Enr Enrolled a at Boone H one Hospital f for 12 12 week eek p pul ulmonary r reh ehab. b. Initially lly, he cou ould ld b barely ly w walk lk 2 minutes c con ontinuou ously, a and couldn’t w coul walk a any m more e than 320 320 fee eet total. He s e sco cored ed 10 0 on RPE n RPE sca cale e –2 minutes of of walk lking He e sco cored ed 4 o 4 on D n DS s sca cale Daily S Sympt ptoms: : cough, gh, sp sputum, w whe heezing, d dysp yspnea *rating o of perceived e ed exertion on *dysp spnea sc scal ale
PRIOR TO PULMONARY REHAB Patient t sco cored 30 30 on n CO COPD A D Assessment T Test (CA CAT) This is t the highest you ou can scor ore and it me means that the sym ymptom oms e experienced b by y the patient are severe and pa nd it a also indicates t that they w woul uld b bene nefit from pul pulmonary reh ehab ab, ad addition o of other er med medications, an and man manage age exac xacer erbat ations.
WHAT DOES >30 ON CAT MEAN? Their condition stops them doing everything they want to do. They never have any good days. If they can manage to take a bath or shower, it takes them a long time. They cannot go out of the house for shopping or recreation, or do their housework. Often, they cannot go far from their bed or chair. They feel as if they have become an invalid.
PR--GRADUATION Midway through, he was a able to o do o 5min. In Interval exercises for or a total of of 25 minutes By t y the end of of 1 12 w weeks, he w was able t to o do 12 12 minute i interval f for r a tota tal o of 48 f 48 minutes up t up to 13 1320 f 0 feet. His RPE PE was as under er 4 4 His D DS S sc scale w was s unde der 2
GOALS OF PR Pr Preven ent s symptoms an and exac xacer erbations Impr prove A ADL DLs and nd Q QOL. Educate p patient abou out t the disease Tobacco c cessation c coun unselling Enc ncourage pa patient to pa participate i in n therapy a and nd c cont ntinue at home a after f formal therapy. y.
CURRENTLY 2 years later, h his c cond ndition c cont ntinued t to worsen and nd had a doub uble pne pneum umonectomy in n 7/ 7/20 2017 9/ 9/20 2017-- ---he was r readmitted t to t o the h hos ospital for or g grade 2 2 rejection on 3 weeks after trans nsplant nt After s stabilization and recovery, he was sent b back to o pulmon onary y rehab for or cond nditioning. Patient i is n now d doing well. ll.
REFERENCES Global l Initiative f for Chronic O Obstructive L Lung Disease ( (GOLD LD): G Global l Str trategy f for th the Diagnosis, Mana nagement, a and nd P Prevention o of C COPD 2017. www.goldco dcopd. d.org The a association n betw tween d daily e exacerbation sym ymptoms and nd p phys ysical a activity in n pati tients w with th c chroni nic obstructive pul ulmonary y diseas ase Int J J Chron Obstr truct t Pulmon D Dis. 20 2018 J 8 Jul 18; 8;13:2199 99-22 2206 06. d doi oi: 10.2147/COPD. D.S156986. e eCollection on 2018. ATS Committee o on n Proficiency S y Sta tand ndards for Clinical P Pul ulmona nary F y Func unction Lab aboratorie ies. A ATS s S statement: g guid idelines for t the s six ix-mi minute e walk t test. t. A Am J RespirCritCare M Med 2002; 2002; 1 166: 66:111. COPD spectr trum d m diagram-courtesy o of med medscape pe i ima mages.
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries