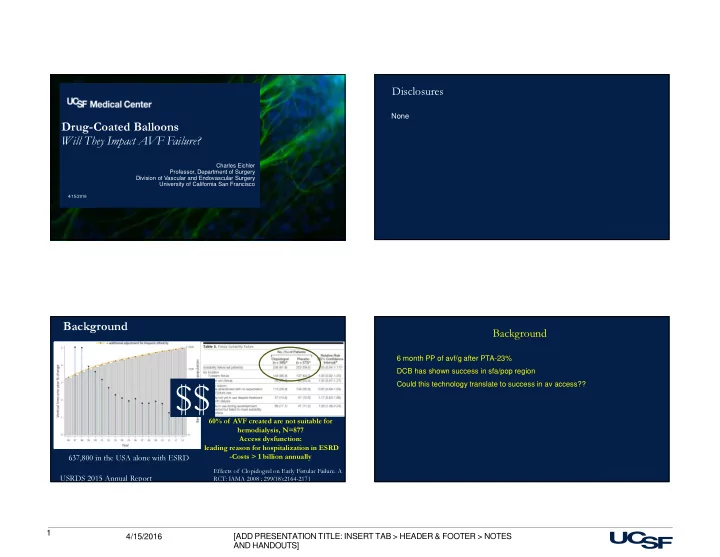
$$ 60% of AVF created are not suitable for hemodialysis, N=877 - PowerPoint PPT Presentation
Disclosures None Drug-Coated Balloons Will They Impact AVF Failure? Charles Eichler Professor, Department of Surgery Division of Vascular and Endovascular Surgery University of California San Francisco 4/15/2016 2 Presentation Title and/or
Disclosures None Drug-Coated Balloons Will They Impact AVF Failure? Charles Eichler Professor, Department of Surgery Division of Vascular and Endovascular Surgery University of California San Francisco 4/15/2016 2 Presentation Title and/or Sub Brand Name Here 4/15/2016 Background Background � 6 month PP of avf/g after PTA-23% � DCB has shown success in sfa/pop region � Could this technology translate to success in av access?? $$ 60% of AVF created are not suitable for hemodialysis, N=877 Access dysfunction: leading reason for hospitalization in ESRD -Costs > 1 billion annually 637,800 in the USA alone with ESRD Effects of Clopidogrel on Early Fistular Failure. A 4 4/15/2016 USRDS 2015 Annual Report RCT: JAMA 2008 ; 299(18):2164-2171 1 [ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES 4/15/2016 AND HANDOUTS]
Failure Mode of AVF Treatment of the failing AVF Pre-existing vein disease � Balloon angioplasty � PTA denudes endothelial cells and Swing segment injury tears the intima and media (perforation) � Cutting balloons help to some extent Decreased vasorelaxing factors (nitric � Elastic recoil following balloon oxide) deflation � Vonatanapase – pancreatic High shear stress, vortices, and eddy elastase currents � Bare metal Stents � Viabahn stent graft The net result of these injuries are tissue � Offers marginally improved patency inflammation, growth factor production, at 6 months. matrix synthesis & cellular proliferation. � costly Dolmatch, Ross and others. NEJM 362;6:2010 Drug Coated Balloons Current treatment produces more injury to Microtubules Are the healing AVF resulting in increased Thermodynamically cellular proliferation and high rates of In A State Of restenosis Dynamic Instability Combining a high pressure balloon with the anti-proliferatve drug paclitaxel offers sufficient mechanical dilation of the venous Life Between stenosis with pharmacologic inhibition of Catastrophe And proliferation resulting in increased AVF Microtubule formation is dependent on the GTP -> Rescue GDP energy associated with the β tubulin polymer patency Kinetochore Spindle apparatus during mitosis. Paclitaxel binds to the inside of β tubulin and 7 Spindle is formed from microtubules prevents microtubule dissassembly 2 [ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES 4/15/2016 AND HANDOUTS]
Paclitaxel concentrations following DCB treatment of Medtronic Im.Pact Admiral porcine iliac arteries. Unclear to the concentration in venous tissue at this time 10 ration ng/mg) 80 PTX Concentration Excipient urea 1 (ng/mg) 60 0.1 0.01 40 EC 50 Paclitaxel Paclitaxel Conc 0.001 BARD 035 Lutonix 60 90 120 150 180 20 Time [Days] Nominal Dose Porcine IleoFemoral Artery 0 3X Safety Margin Dose 0 50 100 150 200 Days Detectable levels of drug in tissue over 180 days in both arms (therapy dose and safety margin). At 320 days, no quantifiable Detectable levels of drug in tissue over 180 days in both arms (therapy dose and safety margin). At 320 days, no quantifiable Polysorbate & Sorbitol drug is identified in the targeted tissue area in nominal dose. Drug concentration levels in plasma are < 1/10 of that in tissue, drug is identified in the targeted tissue area in nominal dose. Drug concentration levels in plasma are < 1/10 of that in tissue, drop 50% in 30 minutes, and not detectable after 48 hours. drop 50% in 30 minutes, and not detectable after 48 hours. Medtronic Data on file Existing Literature – Few Reports - Prospective randomized single-center DCB (n=20, IN.PACT Admiral) v PTA (n=20) for treatment of failed AVF/Gs 1 Goal. To compare the performance of - Prospectively enrolled consecutive patients (n=26) receiving DCB (IN.PACT Admiral) for failed AVFs 2 DCBs v. POBA for the treatment of - venous stenosis of vascular access circuit in patients undergoing hemodialysis Figure: Single patient treated with 7 x 80 mm DCB then 7 1. Katsanos K, et al. J Endovasc Ther 19:263-72 (2012). 2. Patanè D, et al. J Vasc Access 15:338-43 (2014). x 80 Dorado, top panel. Follow up fistulograms every 2 11 4/15/2016 12 Presentation Title and/or Sub Brand Name Here 4/15/2016 months for 6 months, bottom. J Endovasc Ther 2012; 19:263-272 3 [ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES 4/15/2016 AND HANDOUTS]
DCB improved target lesion and dialysis circuit primary patency Decreased repeat procedures 20% v. 65% P=0.002 No benefit to secondary patency High rate of DCB failure meaning that further dilation was necessary 13 Presentation Title and/or Sub Brand Name Here 4/15/2016 14 Presentation Title and/or Sub Brand Name Here 4/15/2016 J Endovasc Ther 2012; 19:263-272 Single center experience using DCB to treat failed radiocephalic AV shunts Prospective consecutive enrollment of 26 patients treated with DCB (IN.PACT Admiral) for failed AVFs 12-mo 1° Patency: DCB 38% v PTA 0% 12-mo 1° Patency: DCB 29% v PTA 14% 12-mo 1° Patency: DCB 35% v PTA 5% (p<0.001) (p=0.003) (p=0.26) Kitrou PM, et al., continued follow-up of the original report demonstrate higher TL 1° Patency in DCB arm v PTA arm (left), as well as for both AVGs (center, n=13) and AVFs (right, n=13). 1. Kitrou PM, et al. Eur J Radiol 84:418-23 (2015). 1. Patanè D, et al. J Vasc Access 15:338-43 (2014). 15 Presentation Title and/or Sub Brand Name Here 16 4/15/2016 4 [ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES 4/15/2016 AND HANDOUTS]
Review-upcoming in J of Vasc Access � 6 published studies on 254 interventions � 2 randomised and 4 cohort studies � Wasting of the DEB reported in two studies-55% of patients � At 6 mon, TL PP 70% to 97% for DCB vs 0% to 26% for PTA TL 1° Patency TL 2° Patency 6-mo 92.3% (24/26) 12-mo 90.9% (20/22) 100.0% (20/20) 24-mo 57.8% (11/19) 94.7% (18/19) 1. Patanè D, et al. J Vasc Access 15:338-43 (2014). 17 4/15/2016 18 Presentation Title and/or Sub Brand Name Here 4/15/2016 Summary of Key Findings Cephalic vein stenosis in a patient on HD treated by a 6 mm x 80 mm 035 Impact Looking Ahead � Current literature landscape consists of single center DCB. Treatment was 6 month ago and AVF functioning well with no restenosis prospective and retrospective studies - Data are limited reporting use of DCB for AVF/G restenosis � Results are promising despite challenging application - Only US RCT investigating DCB is ongoing (Bard Lutonix 035; enrollment and patient profile complete) � Current devices studied are lower extremity devices used - Existing device configurations directed to lower extremity intervention in AVF applications - Until larger series demonstrate cost-effectiveness, DCB configurations and � A need exists for larger, multicenter studies employing adoption for AVF/G revision may be limited AVF-configured devices (>7mm diameter) 19 4/15/2016 5 [ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES 4/15/2016 AND HANDOUTS]
Thank you for your attention 6 [ADD PRESENTATION TITLE: INSERT TAB > HEADER & FOOTER > NOTES 4/15/2016 AND HANDOUTS]
Recommend








More recommend
Explore More Topics
Stay informed with curated content and fresh updates.