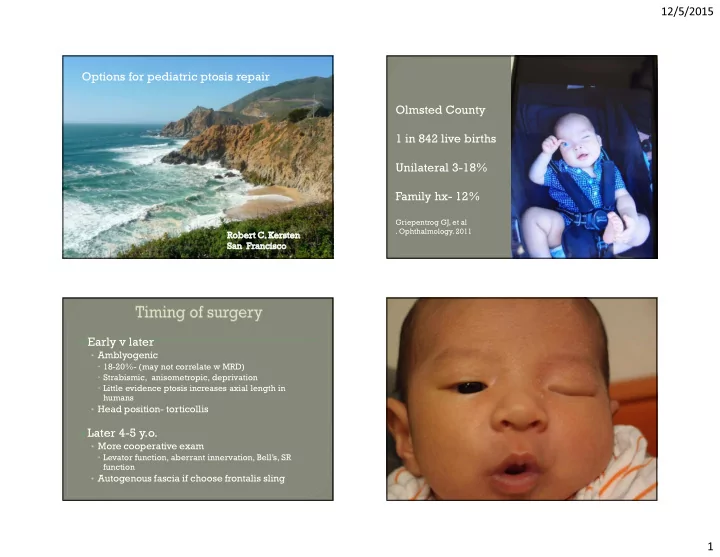
12/5/2015 Options for pediatric ptosis repair Olmsted County 1 in 842 live births Unilateral 3-18% Family hx- 12% Griepentrog GJ, et al . Ophthalmology. 2011 � Early v later • Amblyogenic � 18-20%- (may not correlate w MRD) � Strabismic, anisometropic, deprivation � Little evidence ptosis increases axial length in humans • Head position- torticollis � Later 4-5 y.o. • More cooperative exam � Levator function, aberrant innervation, Bell’s, SR function • Autogenous fascia if choose frontalis sling 1
12/5/2015 � Levator function � Amblyopia � Aberrant innervation levator (Marcus-Gunn, III n palsy) � Good function: > 10 mm • Mullerectomy, Fasanella-Servat (2 mm ptosis, excellent function) • Aponeurotic advancement- goal- height under anesthesia � Intermediate: 6-8 mm • Levator advancement plus tarsectomy � Poor: < 6 mm • Frontalis sling • Supramaximal resection � (20-30 mm levator muscle) : 2
12/5/2015 3 y.o.- comngenital ptosis L.U.L. Astigmatism O.D.- part time occlusion 2-3 m m function Poor levator function: Generally “bypass” levator muscle Sling materials: •Frontalis sling- effectively transmits force from frontalis muscle to eyelid •Autogenous fascia* •Homologous fascia •Open lid crease •PTFE- suture or patch* •Suture sling directly to tarsus •Supramid •Frontalis muscle •Adjust lid contour with tarsal sutures advancement(?) •Mersilene mesh •Fixate crease •Proline suture •Adjust height with tension at brow incision •Silicone tube 3
12/5/2015 Frontalis sling allows more efficient frontalis elevation of eyelid Reflex recruitment of frontalis muscle to clear visual axis 1:1 elevation of eyelid : brow 4
12/5/2015 5
12/5/2015 Congenital nil function ptosis s/p PTFE sling Recruiting frontalis muscle 6
12/5/2015 Congenital R. III n palsy s/p extirpation R levator unilateral fascia lata sling Levator ablation: unpredictable, undesirable levator 7
12/5/2015 Unilateral ptosis: unilateral vs Bilatera l ptosis bilateral surgery Frontalis sling- “self-adjusting ” Variable recruitment of frontalis to clear � Amblyopia- no drive to recruit frontalis � Results in more lagophthalmus • Avoid if no Bell’s � Not useful if aberrant innervation of levator • Marcus-Gunn jaw wink • Congenital III n palsy w aberrant innervation 8
12/5/2015 3 y.o- poor function ptosis, amblyopia w no frontalis recruitme Good SR function, good Bell’s 9
12/5/2015 10
12/5/2015 11
12/5/2015 12
12/5/2015 � Early v later • Amblyogenic � Head position- tortocollis � Later 4-5 y.o. � Options • Levator surgery • Frontalis sling � Poor/aberrant levator function � Bypass levator w sling • Ineffective if amblyopia � Supramaximal resection • Avoid if aberrant innervation • Exposure greater concern post-op � Avoid if poor Bell’s � “Double –elevator palsy” 13
12/5/2015 14
12/5/2015 15
12/5/2015 16
12/5/2015 17
12/5/2015 18
12/5/2015 19
12/5/2015 Robert C. Kersten M.D. Kerstenr@vision.ucsf.edu O-415-353-9399 C-415-235-0227 20
12/5/2015 External DCR- still my preference Robert C Kersten UCSF Robert C. Kersten M.D. Kerstenr@vision.ucsf.edu O-415-353-9399 C-415-235-0227 The relation of Graves Hyperthyroidism and Graves Ophthalmopathy Robert C. Kersten UCSF 21
12/5/2015 � Early v later • Amblyogenic � 18-20%- (may not correlate w MRD) � Strabismic, anisotropic, deprivation • Head position- torticollis • Little evidence ptosis increases axial length in humans � Later 4-5 y.o. • More cooperative exam • Autogenous fascia if choose frontalis sling 22
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries