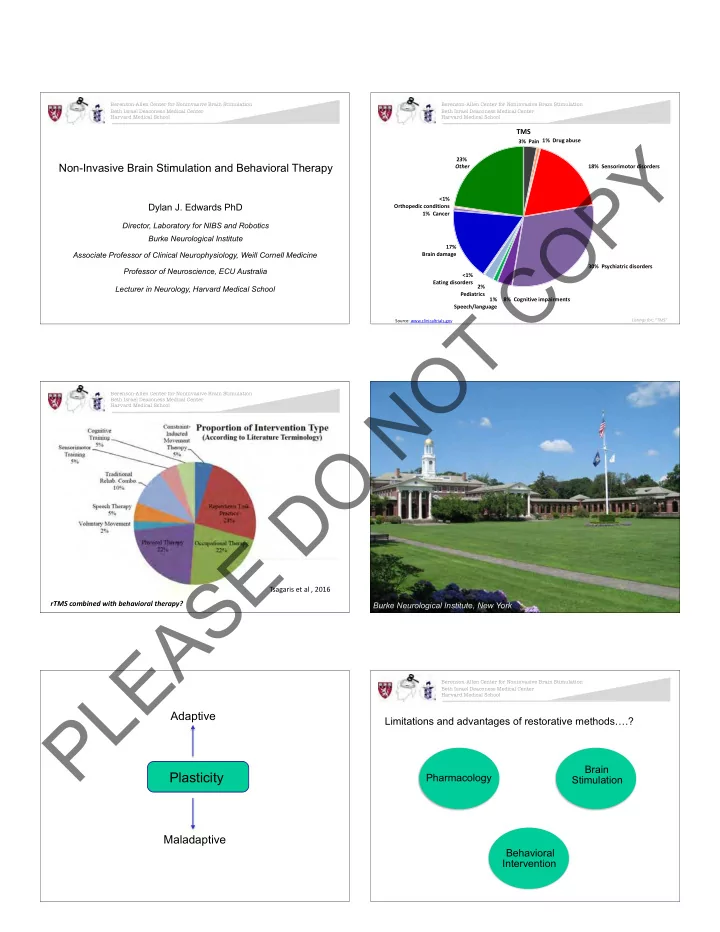
Berenson-Allen Center for Noninvasive Brain Stimulation Berenson-Allen Center for Noninvasive Brain Stimulation Beth Israel Deaconess Medical Center Beth Israel Deaconess Medical Center Harvard Medical School Harvard Medical School TMS Y 3% Pain 1% Drug abuse 23% Non-Invasive Brain Stimulation and Behavioral Therapy Other 18% Sensorimotor disorders P <1% Dylan J. Edwards PhD Orthopedic conditions O 1% Cancer Director, Laboratory for NIBS and Robotics Burke Neurological Institute 17% C Brain damage Associate Professor of Clinical Neurophysiology, Weill Cornell Medicine 30% Psychiatric disorders Professor of Neuroscience, ECU Australia <1% Eating disorders 2% Lecturer in Neurology, Harvard Medical School Pediatrics 1% 8% Cognitive impairments T Speech/language Listings for; “TMS” Source: www.clinicaltrials.gov O N Berenson-Allen Center for Noninvasive Brain Stimulation Beth Israel Deaconess Medical Center Harvard Medical School O D E S Tsagaris et al , 2016 rTMS combined with behavioral therapy? A Burke Neurological Institute, New York E L Berenson-Allen Center for Noninvasive Brain Stimulation Beth Israel Deaconess Medical Center Harvard Medical School P Adaptive Limitations and advantages of restorative methods … .? Brain Plasticity Pharmacology Stimulation Maladaptive Behavioral Intervention
Smaller Coil Y P How does repetitive behavior affect motor cortex? Focality / O Specificity C Network activation T O N O D Motor map changes with skilled practice E S Simple repetitive finger movements increase excitability A E TMS Demonstration L P How does NIBS affect motor cortex?
Physiology of TMS SICF Berenson-Allen Center for Noninvasive Brain Stimulation Beth Israel Deaconess Medical Center Harvard Medical School Magstim Magstim Magstim Magstim ADULT M1 Y Stimulating coil Stimulating coil TMS P 1.5 msec. ) ( ) ( Amplitude (% control) α α 300 Hallett, 2000 250 O Muscle Spinal recordings 200 150 I-waves 100 Ramón y Cajal C Periodicity ~ 1.5ms 50 1 1.5 2 2.5 3 3.5 4 4.5 5 Inter-stimulus Interval (ms) EMG EMG EMG EMG Ziemann et al, 1998 Instrument Instrument Instrument Instrument Di Lazzaro et al. (1998) T O N Rate-dependent TMS protocols “An excited neuron tends to decrease its discharge to inactive neurons, and increase this O High-frequency Excitatory discharge to any active neuron, and therefore to ~10Hz form a route to it, whether there are intervening neurons between the two or not. With repetition, REPETITIVE this tendency is prepotent in the formation of D neural routes”. Low-frequency Inhibitory ~1Hz (Hebb, 1932, p.13). 50Hz williamcalvin.com E Donald Hebb Intermittent Excitatory 5Hz THETA BURST S 2 sec 8 sec The Organisation of Behaviour: A Neuropsychological Theory. D.O. HEBB (1949) Inhibitory Continuous A D Edwards E L Long-term potentiation Long-term potentiation P Pre-synaptic Pre-synaptic Glu Glu Na+ Na+ Ca++ Ca++ Na+ Na+ Mg++ Mg++ NMDA NMDA AMPA AMPA Post-synaptic Post-synaptic ↑ EPSP EPSP Dendritic spine Dendritic spine CaM CaMKII Ca++ AMPA AMPA Thickbroom (2007) Ex Brain Res. Thickbroom (2007) Ex Brain Res.
Berenson-Allen Center for Noninvasive Brain Stimulation LTP/ LTD Beth Israel Deaconess Medical Center Harvard Medical School Long-term depression Y Glu P Ca++ O Mg++ NMDA AMPA C CaMKII CaM Ca++ C PP2B N Webster et al (2006) Clinical application - rTMS, Stroke Motor Recovery T Thickbroom (2007) Ex Brain Res. O N Functional Improvements TMS correlates sRT/cRT Resting MT O Takeuchi, et al, 2008 Yozbatiran et al, 2009 Pinch force acceleration Transcallosal Inhibition Malcom et al, 2007 Boggio et al, 2007 Hummel et al, 2007 Fregni et al., 2006 fingers/thumb AROM D Talelli et al., 2007 Kim MEP Amplitude Fregni et al., 2005 Movement accuracy et al., 2006 Hummel et Mansur et al., 2005 al, 2006 Khedr et al., Takeuchi et al., 2005 Purdue Pegboard 2005 Hummel et al, Boggio, et al., 2006 E 2005 JTT Werhahn, et al., 2003 Webster et al (2006) Webster et al (2006) S IMPROVED CORTICOMOTOR OUTPUT FROM IPSI-LESIONAL M1 IMPROVED CORTICOMOTOR OUTPUT FROM IPSI-LESIONAL M1 & IMPROVED MOTOR BEHAVIOUR & IMPROVED MOTOR BEHAVIOUR A E L Altering cortical excitability before repetitive synaptic activity P How does combined intervention affect motor cortex? • 1mA 10mins tDCS • rTMS at 5Hz 100stim train at AMT – decreases SICI, but not lasting change in excitability as tested by single pulse TMS • Result= after effects of tDCS can generate opposite effects of rTMS or conversely can alter the after effects of tDCS Lang et al (2004)
Berenson-Allen Center for Noninvasive Brain Stimulation Beth Israel Deaconess Medical Center Harvard Medical School Y P Is coupling NIBS with therapy good? O C T Buch et al 2011, J Neurosci O N Motor systems example If … SICF Berenson-Allen Center for Noninvasive Brain Stimulation Beth Israel Deaconess Medical Center Harvard Medical School Motor Training = improvement in function ‘X’ O and … D NIBS = improvement in function ‘X’ does … E Motor Training = improvement in function + S 2X, X 2 , or 0?? NIBS tDCS A E L Anodal tDCS combined with robotic motor training Berenson-Allen Center for Noninvasive Brain Stimulation Beth Israel Deaconess Medical Center Harvard Medical School P Anodal tDCS combined with robotic motor training 1mV Group SICI Index Conditioned / uncond MEP amplitude * p < 0.05 1 * 0.5 Pre-tDCS Post-tDCS Post-Robot 0 Pre Post Post tDCS tDCS Robot Edwards et al (2009) Edwards et al (2009)
Robotics for assessment of performance kinematics Upper limb robotics at Burke-Cornell, New York Edwards PI: R01 HD069776 Y Pre – training P Post - training O C T Robotics with brain stimulation in patients with motor dysfunction O N TMS Method' Author' Priming'Method' PROTOCOL' Effect' Dura:on' rTMS' Iyer' rTMS%% rTMS% increased%inhibitory%effect% >60%min% % % Daskalakis'' rTMS%% rTMS% no%change% O % % Siebner' tDCS% rTMS% no%change% 20%min% % % Siebner' tDCS% rTMS% reversed%results%in%MEP% 20%min% voluntary%% D TBS' Iezzi' (finger%abduct'n)%*% cTBS% reversed%results%in%MEP% >30%min% voluntary%% % % lezzi' (finger%abduct'n)%*% iTBS% %reversed%results%in%MEP% >30%min% PAS' Muller' N20H5ms% N20+2ms% priming%produced%increase%in%MEP% >30%min% priming%had%no%effect%on%MEP% E % % Muller' N20+2ms% N20+2ms% change% >30%min% % % Zienman' voluntary%*% N20H5% enhanced%inhibiLon% % % Zienman' voluntary%*% N20+2ms% no%change% S *%presumed%excitaLon% Prelim data for Nexstim NICHE Trial Inhibitory% ExciLtory%% A E L Repetitive Transcranial Magnetic Stimulation (rTMS) P Aiming tool: centering, rotation, tilting Nexstim NICHE Trial 2014-16 Electrical field display Clinicaltrials.gov # NCT02089464 Parameters: PI: Richard Harvey RIC • 900 pulses • 1 Hz rTMS (inhibitory) to M1 of non-lesioned hemisphere • 110% of motor threshold for Extensor Digitorum Communis Patient set up (m.EDC)
Task Oriented Rehabilitation Nexstim NICHE Trial 2014-16 Clinicaltrials.gov # NCT02089464 Patient Goals: Y • Cut food with knife & fork International Stroke Conference Feb 2017 Announcement • Cook • Reach for items above shoulder height P • Fasten clothing (buttons, zippers, laces) • Hold grandchild Mean change across both groups (n ~150): • Hold tools in affected hand O UEFM was 8.2 points • Driving • Golf *no difference between sham and real groups C Person Source: www.nexstim.com/news-and-events/press-releases/2017/ Environment Occupation Collaborative process between therapist T and patient O N How does unaffected M1 excitability relate to hemiparesis? O Ac#ve&coil& Sham&Coil& D E S A E L P Aaron Boes MD PhD BIDMC/MGH/UIOWA A C Mike Fox MD PhD BIDMC/MGH/Harvard B D Amy Kuceyeski, Ph.D. Radiology and Neuroscience, ! Figure'4.'Sample'data'for'pa3ent'with'cor3cal/subcor3cal'stroke'(A)'axial'T1'MRI'with'leE'cor3cal/subcor3cal' Weill Cornell
Berenson-Allen Center for Noninvasive Brain Stimulation n=103 Beth Israel Deaconess Medical Center Harvard Medical School VLSM in 3-12month Post-Stroke (hemiparesis) Y P O Other cortical areas? C Hot colour = maximum overlap for unaffected hemisphere hyper-excitability Courtesy A .Boes MD March 2017 T O N Evidence / Rationale Elsner B, Kugler J, Pohl M, Mehrholz J (2013) Transcranial direct current stimulation (tDCS) for improving aphasia in patients after stroke (Review). O Cochrane Database Syst Rev 6:CD009760. No evidence for tDCS as useful adjunct some merit in cathodal stimulation? D Post-stroke aphasia? Thiel et al (2013). Evidence of NIBS on language networks and recovery in early post-stroke aphasia. E How is the network disrupted? R hem1 Hz rTMS + SL therapy improves language recovery Is NIBS useful? Webster et al (2006) Can it be effectively combined with SL therapy? and favors L hem language network activation S A E L + + Repetitive transmagnetic stimulation (rTMS) Subject 1 P Infarct Aiming tool: centering, rotation, tilting Electrical field display Parameters: Pars triangularis • 900 pulses • 1 Hz rTMS (inhibitory) to pars triangularis of non-lesioned hemisphere • Motor threshold determination with First dorsal interosseus muscle • Real - 90% RMT • Sham – 10% RMT Patient set up CIHR: MOP-286185
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries