The silent reflux: esophagus and diabetes
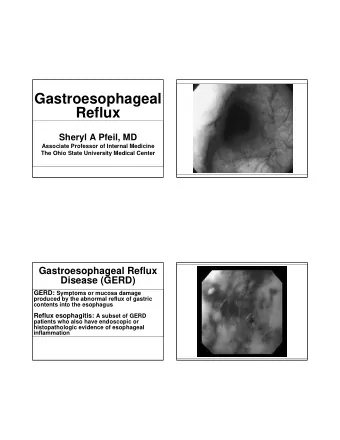
GERD is caused by compromised esophageal defense mechanisms, including reduced bicarbonate production, and an abnormality of the lower esophageal sphincter, that produce a reflux of gastric contents from the stomach into the esophagus
What is silent/extra-esophageal reflux GERD is among the most common diseases encountered by primary � care physicians and gastroenterologists. The predominant symptoms of GERD are heartburn and � regurgitation; however, patients may also present with atypical symptoms. These are often referred to as extraesophageal manifestations of � GERD. Extraesophageal reflux (EER) symptoms can occur with or without � typical GERD symptoms, which, in the latter setting, may delay the diagnosis of reflux Yuksel ES, et al. New developments in extraesophageal reflux disease. Gastroenterol Hepatol (N Y). 2012 Sep; 8(9): 590–599.
Typical laryngopharyngeal reflux (LPR) symptoms Hoarseness / dysphonia (71%) � Cough (51%) � Globus pharyngeus (throat lump sensation) (47%) � Frequent throat clearing (42%) � Mild dysphagia / posterior pharynx edema (35%) � Wheezing � Sore throat � Excessive throat mucus � Post-nasal drip � Post-prandial rhinorrhea � Laryngoscope 1991;101:1 Am J Gastroenterol 1990;85:38-40 Ear, Nose & Throat Journal 2002;81(Suppl 2):14-18
The Montreal definition of constituent syndromes of extraesophageal reflux Yuksel ES, et al. New developments in extraesophageal reflux disease. Gastroenterol Hepatol (N Y). 2012 Sep; 8(9): 590–599.
Uncommon symptom in LPR HEARTBURN � − Hence, 'silent reflux' Only 35% of patients with LPR have heartburn; � − Only 25% with esophagitis Up to 38% have normal esophageal pH test � Laryngoscope 1991;101:1 Am J Gastroenterol 1990;85:38-40 Ear, Nose & Throat Journal 2002;81(Suppl 2):14-18
LPR complications Adult-onset asthma � Interstitial lung disease � Recurrent bronchitis � Recurrent pneumonia � Recurrent sinusitis � Accelerated loss of tooth enamel � Paradoxical vocal cord dysfunction � Laryngeal spasm � Subglottic stenosis � Vocal cord granulomas and polyps � Laryngeal CA (without history of smoking or alcohol use) � Laryngoscope 1991;101:1 Am J Gastroenterol 1990;85:38-40 Ear, Nose & Throat Journal 2002;81(Suppl 2):14-18
Gastroesophageal reflux disease (GERD) is the third most common cause of chronic cough (after postnasal drip syndrome [PNDS] and asthma). These 3 causes account for 86% of all cases of chronic cough, and there are often multiple causes for each case. Yuksel ES, et al. New developments in extraesophageal reflux disease. Gastroenterol Hepatol (N Y). 2012 Sep; 8(9): 590–599.
Asthma and GERD may exacerbate each other, as GERD may induce bronchospasm, and asthma may induce GERD. Treating both conditions may break this cycle and improve patients’ symptoms. Yuksel ES, et al. New developments in extraesophageal reflux disease. Gastroenterol Hepatol (N Y). 2012 Sep; 8(9): 590–599.
Pathophysiology Direct mechanism: caustic acid and pepsin irritation � − Dense neural blanket in larynx protects against aspiration − Sensory deficit in those with laryngeal edema (reversible) Indirect mechanism: irritation of esophagus evoking laryngeal � reflexes that causes vagally-mediated change (bronchoconstriction/cough and mucus accumulation/throat clearing) Yuksel ES, et al. New developments in extraesophageal reflux disease. Gastroenterol Hepatol (N Y). 2012 Sep; 8(9): 590–599.
How does LPR cause damage Larynx has no intrinsic defense or clearance mechanisms. � Gastric acid exposure. � Pepsin activation at pH < 6.5 � pH < 4 – mucosal damage � Pepsin inactivated at pH of 8 � Lingering pepsin can be reactivated within 24 hours � Laryngoscope 1991;101:1 Am J Gastroenterol 1990;85:38-40 Ear, Nose & Throat Journal 2002;81(Suppl 2):14-18
Risk factors Obesity or acute weight gain: increase intra-abdominal pressure � Gastroparesis: diabetes, pre-diabetes, narcotics use, hypothyroidism, � idiopathic Habitual and volitional excessive gastric distension syndrome � Aerophagia and carbonated beverages: delivery of gastric acid and � enzymes to LP with each burp or belch Hiatal hernia, alcohol, caffeine, peppermints, and chocolates: lowers � resting tone of the upper and lower esophageal sphincters Laryngoscope 1991;101:1 Am J Gastroenterol 1990;85:38-40 Ear, Nose & Throat Journal 2002;81(Suppl 2):14-18
Risk factors Acidic and spicy foods: causes direct irritation and inflammation � Nicotine: stimulates acid production � Singing, heavy lifting, exercise, and bending over: prolonged duration � and high magnitude of increases in intra-abdominal pressure Gastric outlet obstruction / malignancy � Sleep apnea � Laryngoscope 1991;101:1 Am J Gastroenterol 1990;85:38-40 Ear, Nose & Throat Journal 2002;81(Suppl 2):14-18
Diagnosis of LPR Yuksel ES, et al. New developments in extraesophageal reflux disease. Gastroenterol Hepatol (N Y). 2012 Sep; 8(9): 590–599.
Treatment of LPR PPI therapy is the standard of care when GERD is suspected to be � the etiology of chronic throat symptoms. Patients who are unresponsive to PPI therapy may have either non- � reflux-related causes or a functional component to their symptoms. Continued acid and/or pepsin-related injury to the larynx is the cause � of symptoms, despite a lack of response to PPI therapy. Yuksel ES, et al. New developments in extraesophageal reflux disease. Gastroenterol Hepatol (N Y). 2012 Sep; 8(9): 590–599.
Non-response to PPI therapy Proton pumps in laryngeal seromucinous glands and duct cells may � play a role in the pathogenesis of LPR signs and symptoms. Laryngeal proton pumps may activate in response to reflux or other � causes of inflammation or infection in order to preserve intracellular pH and, thus, viability. An alternative explanation for the lack of response to PPI therapy in � LPR patients is that reflux may be intermittent and/or may occur in low volumes. Yuksel ES, et al. New developments in extraesophageal reflux disease. Gastroenterol Hepatol (N Y). 2012 Sep; 8(9): 590–599.
Non-response to PPI therapy (Contd..) Therefore, patients who are suspected of having LPR but who do not � have any warning symptoms or signs should initially be treated with empiric PPI therapy for 1–2 months. If symptoms improve, the therapy may need to be prolonged for up to � 6 months to allow healing of laryngeal tissue. After this time, the dosage should be tapered to the smallest amount � that still results in continued response. In unresponsive patients, impedance and/or pH monitoring may be � the best alternative to rule out reflux as the cause of continued symptoms and to move forward by considering other causes. Yuksel ES, et al. New developments in extraesophageal reflux disease. Gastroenterol Hepatol (N Y). 2012 Sep; 8(9): 590–599.
Silent reflux in diabetes
Differences in individual upper (A) and lower (B) gastrointestinal symptoms between diabetic patients and control groups Diabetic patients have a higher frequency of globus, heartburn and dysmotility like dyspepsia than the controls There was no difference for any item of the lower GI symptoms between the two groups Kim JH , et al. World J Gastroenterol 2010 April 14; 16(14): 1782-1787
Prevalence of esophageal motor dysfunction in diabetics Mandelstam and Lieber were the first to survey a group of diabetics � for evidence of esophageal involvement. They reported that the emptying of barium from the esophagus was � delayed in nearly all diabetics with peripheral neuropathy. Later, they found that this group also exhibited a decrease in the � frequency of peristaltic contractions after swallowing. 80 percent of diabetics with peripheral neuropathy have abnormal � esophageal motility. Only 20 percent of diabetics without neuropathy have abnormal � esophageal motility Ippoliti A. Esophageal disorders in diabetes mellitus. The yale journal of biology and medicine 56 (1983), 267-270
Esophageal changes in diabetes In general, the esophageal changes in diabetes can be described as � a loss of motility. − Pressures are lower in the smooth muscle portion of the esophagus. The amplitude of esophageal body contractions tends to be low, as does the lower esophageal sphincter pressure. − The velocity of esophageal body contraction is reduced. The time required for peristalsis to sweep down the esophagus is prolonged. − The pattern of esophageal body contractions may show the following: absence of contraction after swallowing, and simultaneous or repetitive body contractions. Ippoliti A. Esophageal disorders in diabetes mellitus. The yale journal of biology and medicine 56 (1983), 267-270
Clinical features of esophageal motor dysfunction in diabetes The esophageal motility changes of loss of peristalsis and delayed � transit would be likely to produce dysphagia or esophagitis. The latter is theorized, since impaired clearance of acid is an � important feature of reflux esophagitis. However, most studies agree that esophageal symptoms are quite � uncommon in diabetics. Ippoliti A. Esophageal disorders in diabetes mellitus. The yale journal of biology and medicine 56 (1983), 267-270
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries