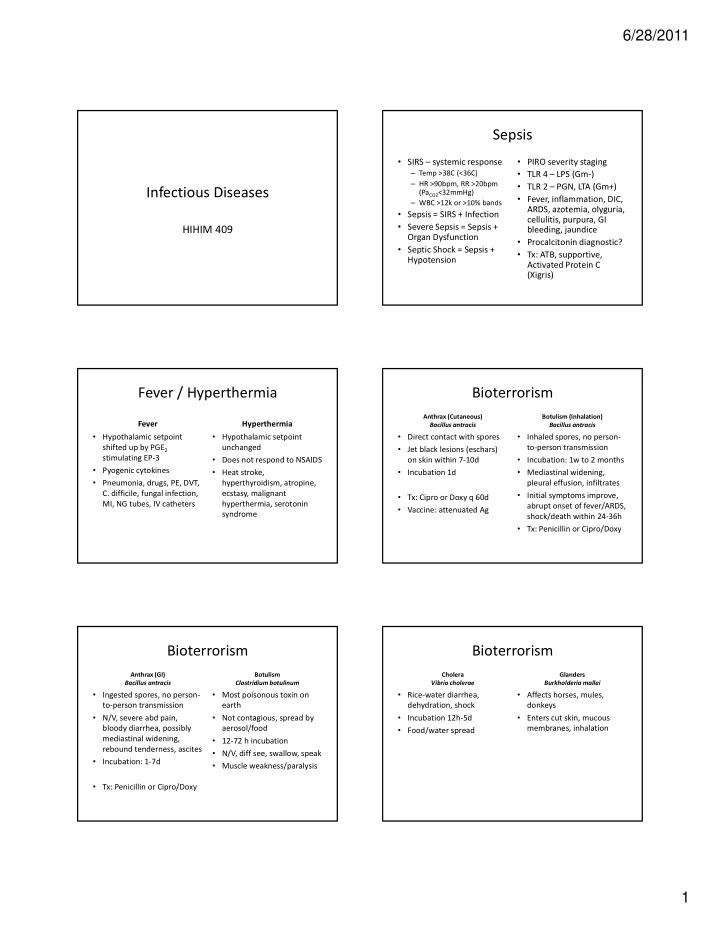
6/28/2011 Sepsis • SIRS – systemic response • PIRO severity staging – Temp >38C (<36C) • TLR 4 – LPS (Gm ‐ ) – HR >90bpm, RR >20bpm • TLR 2 – PGN, LTA (Gm+) Infectious Diseases (Pa CO2 <32mmHg) • Fever, inflammation, DIC, – WBC >12k or >10% bands ARDS azotemia olyguria ARDS, azotemia, olyguria, • Sepsis = SIRS + Infection cellulitis, purpura, GI • Severe Sepsis = Sepsis + HIHIM 409 bleeding, jaundice Organ Dysfunction • Procalcitonin diagnostic? • Septic Shock = Sepsis + • Tx: ATB, supportive, Hypotension Activated Protein C (Xigris) Fever / Hyperthermia Bioterrorism Anthrax (Cutaneous) Botulism (Inhalation) Fever Hyperthermia Bacillus antracis Bacillus antracis • Hypothalamic setpoint • Hypothalamic setpoint • Direct contact with spores • Inhaled spores, no person ‐ shifted up by PGE 2 unchanged to ‐ person transmission • Jet black lesions (eschars) stimulating EP ‐ 3 • Does not respond to NSAIDS on skin within 7 ‐ 10d • Incubation: 1w to 2 months • Pyogenic cytokines • Heat stroke, • Incubation 1d • Mediastinal widening, • Pneumonia, drugs, PE, DVT, hyperthyroidism, atropine, pleural effusion, infiltrates C. difficile, fungal infection, ecstasy, malignant • Initial symptoms improve, • Tx: Cipro or Doxy q 60d MI, NG tubes, IV catheters hyperthermia, serotonin abrupt onset of fever/ARDS, • Vaccine: attenuated Ag syndrome shock/death within 24 ‐ 36h • Tx: Penicillin or Cipro/Doxy Bioterrorism Bioterrorism Anthrax (GI) Botulism Cholera Glanders Bacillus antracis Clostridium botulinum Vibrio cholerae Burkholderia mallei • Ingested spores, no person ‐ • Most poisonous toxin on • Rice ‐ water diarrhea, • Affects horses, mules, to ‐ person transmission earth dehydration, shock donkeys • N/V, severe abd pain, • Not contagious, spread by • Incubation 12h ‐ 5d • Enters cut skin, mucous bloody diarrhea, possibly aerosol/food membranes, inhalation • Food/water spread mediastinal widening, • 12 ‐ 72 h incubation rebound tenderness, ascites • N/V, diff see, swallow, speak • Incubation: 1 ‐ 7d • Muscle weakness/paralysis • Tx: Penicillin or Cipro/Doxy 1
6/28/2011 Bioterrorism Bioterrorism Plague Q Fever Smallpox Tularemia Yrsinia pestis Coxiella burnetii Variola major Francisella tularensis • “Black Death”, infected fleas • Nonspecific febrile • Officially eradicated • One of most infectious • Bubonic – 1 ‐ 10 cm buboes on syndrome, pneumonia bacteria in world • Incubation 10 ‐ 14d skin w/ edema, flu ‐ like symptoms w/ abd pain • Hepatitis, endocarditis, • Tick/insect bites • High fever, HA, backache, g , , , • Septicemic ‐ secondary granulomatous vomiting, rash on palm/sole • Incubation 10 ‐ 14d septicemia, thromboses in complications acral v. leading to necrosis • Highly contagious • Fever, chills, HA, cough, • Tx: Doxycycline 14 ‐ 21d • Penumonic – acute fulminant lethargy, skin ulcers, lymph ‐ • No tx, vaccine within 3 ‐ 5d symptoms, nearly 100% adenopahty mortality rate • Tx: Streptomycin or Doxycycline Bioterrorism Bioterrorism GB VX Ricin Sarin • Binary weapon – two non ‐ • 1000x more toxic than GB • Waste leftover from lethal reagents mix to form processing castor beans • Persists in soil for 6d sarin gas • V/D, dehydration, • Binary weapon y p • Inhibit ACHe, phosphonate hypotension, hallucinations, • Inhibits ACHe, phosphonate esters, light brown oil seizures, hematuria, esters, light brown oil multiple organ dysfunction • If mild: dim vision, • If severe: stop breathing, salivation, chest tightness paralysis, seizures, LOC • No tx available • Tx: Atropine and 2PAMCl Bioterrorism Bioterrorism • Needs Immediate Treatment, Suspect … • “Active” Research • “Secretly” Developing – Algeria – China – Respiratory Symptoms – Egypt – Russia • Acute: Cyanide – India • “Former” Programs – Also nerve agents, mustard, lewisite, phosgene, SEB – Iran Iran • Delayed: Anthrax, Plague, Tularemia D l d A h Pl T l i – Canada d – Israel – Also Q Fever, SEB, ricin, mustard, lewisite, phosgene – France – Neurological Symptoms – N. Korea – Germany – Pakistan • Acute: Nerve agents – Japan – Syria – Also cyanide – S. Africa • Delayed: Botulism – Taiwan – UK, US – Also VEE ‐ CNS 2
6/28/2011 Immunocompromised Complement Deficiency • Deficiencies in • Clues • Hereditary angioedema • DAF and CD59 – Complement – Recurrent Neisseria inf – C1 inhibitor deficiency – Paroxymal nocturnal hemoglobinuria – IG/B ‐ Cell – Recurrent pneumonia – Overactive complement • C1, C3, C4 deficiency – Phagocyte – Severe presentation – Minor stressors trigger attacks – T ‐ cell – Pneumocystis jiroveci – Recurrent pyogenic sinus and respiratory infection • C5 ‐ 9 Deficiency – Burkholderia cepacia • C1q deficiency – Non ‐ TB Mycobacteria – MAC lysis defect – Aspergillus – Neisseria bacteremia – 90% have SLE Ig/B ‐ Cell Deficiency Neutrophil Deficiency • (Bruton’s) X ‐ Linked • CVID • Neutropenia • Hereditary Cyclic N. Agammaglobulinema – Low Ig, normal B ‐ cell – Causes – AD, ELA2 mutation – Btk defect, no B ‐ cells, Ig – Recurrent sinus, • Blacks have lower counts – Predictable cycles respiratory infections – Multiple pyogenic • Chemotherapy patients infections – Chronic infections with – Aphtous stomatitis Giardia, Campylobacter Giardia, Campylobacter • Post ‐ infection, sepsis , p – No live vaccines! No live vaccines! – Tx: G ‐ CSF, steroids T G CSF t id – Tx: ATB, IVIg • Sulfa ‐ drugs, β‐ lactams – Tx: IvIg • Chediak ‐ Higashi • IgA deficiency • Hyper IgM Syndrome – Infections Syndrome – Associated with CVID – X ‐ linked, normal B ‐ cell • Mucositis – Compensated by others – AR, LYST mutation – Low Ig but high IgM • Ecthyma gangrenosum • Secondary Ig deficiencies – Pneumocystis infections • Disseminated candidiasis – Giant lysosomes, – T ‐ cells lack CD40L – Multiple myeloma, • Aspergillosis ineffective granulopoiesis leukemia, skin burns – Oculocutaneous albinism Neutrophil Deficiency Spleen “Deficiency” • Splenectomy • Decrease in circulating • Job’s Syndrome • CGD activated B ‐ cells (75%) – Trauma, ITP, Hairy cell – Hyper IgE, impaired – Defective NADPH leukemia, abscess • Risk of thalassemia > chemotaxis oxidase, no respiratory • Hyposplenism hodgkins > sphero ‐ burst, no killing – STAT3 gene mutation cytosis > ITP > sepsis cytosis > ITP > sepsis – Autoimmune (Graves, Autoimmune (Graves – Infections with catalase I f ti ith t l – Facies, scoliosis, skin Hashimoto, SLE) positive organisms • Infections abscesses, sinusitis – Neoplasia (Hodgkin, – NBT test – S. Pneumoniae (mostly) • Myeloperoxidase (MPO) CML, Sezary) – Haemophilus, GNR, – Makes pus green – Amyloidosis Neisseria (less common) – Converts H 2 O 2 to HOCl – Alcoholism, elderly, Crohn’s, Sickle cell – Deficiency impairs this 3
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries