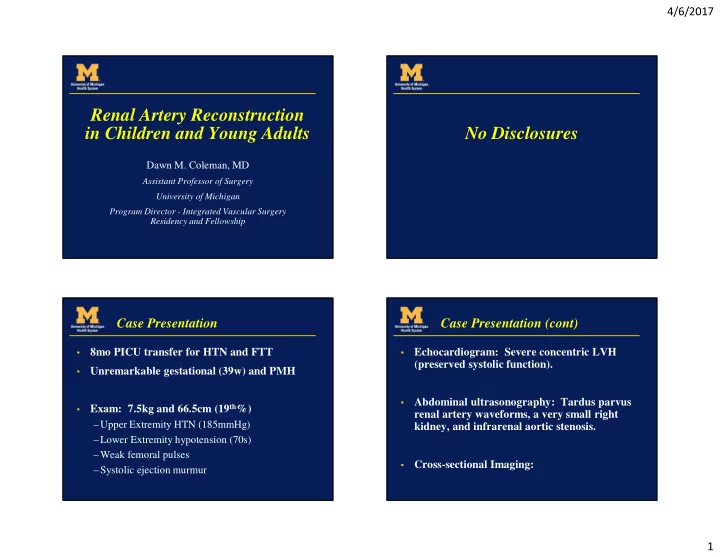
4/6/2017 Renal Artery Reconstruction in Children and Young Adults No Disclosures Dawn M. Coleman, MD Assistant Professor of Surgery University of Michigan Program Director - Integrated Vascular Surgery Residency and Fellowship Case Presentation Case Presentation (cont) 8mo PICU transfer for HTN and FTT Echocardiogram: Severe concentric LVH • • (preserved systolic function). Unremarkable gestational (39w) and PMH • Abdominal ultrasonography: Tardus parvus • Exam: 7.5kg and 66.5cm (19 th %) • renal artery waveforms, a very small right –Upper Extremity HTN (185mmHg) kidney, and infrarenal aortic stenosis. –Lower Extremity hypotension (70s) –Weak femoral pulses Cross-sectional Imaging: • –Systolic ejection murmur 1
4/6/2017 Case Presentation Case Presentation Multiple anti-hypertensives • Progressive abdominal bloating and pain • with SBP <120mmHg Transient azotemia (Cr to 1.54) • Progressive cardiopulmonary failure – • intubated / vent support Phillips et al; Ann Vasc Surg; 2016(3) Aorto-aortic bypass; re-implantation of LRA Case Presentation Uneventful post-op course • D/C POD #18 • –Amlodipine – BP 120/50; Cr 0.1 One year follow-up • –12.6kg (86 th %) –Otherwise stable –Reassuring MRA Phillips et al; Ann Vasc Surg; 2016(3) 2
4/6/2017 Renovascular HTN Pediatric HTN Normal BP: < 90 th % for sex, age, height • Hypertension: Average SBP or DBP ≥ 95 th % • for sex, age, height on at least three separate occasions BP Screening Recommendations: • • ≥ 3 years – any medical setting • < 3 years - congenital heart disease, renal diseases or urologic malformations, hospitalization Pediatric RV HTN Histopathology 3 rd most common cause of HTN in children • (5-10%) Intimal proliferation • Fragmentation of • elastic lamina Associations with: • Medial thinning – NF-1 , William’s Syndrome, Alagille Syndrome, • Tuberous Sclerosis and maternal infection Excessive • –Arteritis periadventitial elastin –Umbilical artery catheterization 3
4/6/2017 Natural History Mid-abdominal Syndrome (MAS) Classified by cephalad • Medically refractory HTN, failure to thrive, • extent of narrowing renal insufficiency and progression to LVH – Suprarenal (69%) –Intrarenal (23%) Life expectancy (untreated) <40 years –Infrarenal (8%) • Thought to arise from • embryonic overfusion of COD: Heart failure, flash pulmonary edema, • the paired dorsal aortas during the 4 th week of hypertensive encephalopathy, stroke/ICH development – 87% renal involvement – 62% splanchnic involvement 5yo with long-segment thoraco-abdominal Diagnostics aortic occlusion; 3-drug HTN + LVH 16mm PTFE Inflammatory work-up (ESR/CRP) • Tunnel anterior to Blood hormone levels (renin) • main pulmonary artery along left lateral Echocardiogram • aspect of heart Renal Duplex • Modest redundancy – 90% Sensitive, 68% Specific for main renal/Ao Retroperitoneal, retro- renal tunnel Cross-sectional Imaging (MRA) • D/C POD 19 with Diagnostic arteriography and renal vein • single drug renin sampling 2y f/u – LVH resolved Castelli et al; Pediatr Radiol; 2014 Coleman et al. JVS 2012;56:482-5. 4
4/6/2017 Indications for Revascularization Medically refractory HTN • Progressive renal insufficiency • NICM (concentric LVH) • Failure to thrive • • 97 patients (58 boys, 39 girls), 3 mos to 17 years Lower extremity sequelae (claudication, • (1963-2006) exertional fatigue, growth disturbance) • 80% developmental renal artery disease • Concurrent disease: Splanchnic arterial occlusive lesions 24% Consider timing and challenges (patient size • Abdominal coarctations 33% and projected growth) J Vasc Surg 2006; 44: 1219-29 UM Experience with RVH - 2006 Options for Reconstruction Renal artery aortic reimplantation (49) • 132 primary operations • Aorto-renal or ilio-renal bypass (40) –13 primary nephrectomies • Extra-anatomic bypass (2) • 30 secondary operations • Segmental reimplantations (7) –9 primary nephrectomies • Arterioplasty (10) • Resection with re-anastomosis (4) • 17 mesenteric revascularizations • Nephrectomy – partial / complete (sub-capsular) • 30 aortic reconstructions • 5
4/6/2017 Patch aortoplasty (PTFE) with 6yo with bilateral ostial RAS visceral revasc. s/p bilateral renal artery reimplantation J Vasc Surg 2002; 35: 560-7 Aorto-aortic bypass (PTFE); retro- Results renal tunnel with visceral revasc. 6
4/6/2017 Technical Pearls Late vein graft aneurysm (8 years) • Single-stage operation • Favor reimplantation • In-vivo reconstruction • Spatulate renal artery-aortic implantantions • Single interrupted sutures with fine monofilament suture (allows for growth) Avoid vein grafts (late • aneurysm) Stanley et al; J Vasc Surg 2006(44) – Hypogastric Artery UM Experience: Endovascular PTA Failures 19 hypertensive patients (ages 2-18)- underwent PTA Neurofibromatosis N=7 Technical success 29 out of 32 lesions (91%) 39% cure, 17% improved, 44% clinical failures J Vasc Interv Radiol 2010; 21:1672-160 7
4/6/2017 18yo – single-drug HTN, failed PTA 10yo, stented for dissection and early stent complicated PTA Stent Extraction and Stent extraction, syndactalization LRA reimplantation and LRA reimplantation Remedial Operations Risk of nephrectomy following PTA and stenting • was 31% (compared to 15% following PTA alone) PTA failures (OSH): Restenosis, thrombosis and • Failures in EV therapy in patients aged <10 years • rupture resulted in a nephrectomy rate of 44% – Time to Failure < 2 years –No nephrectomy following failures in patients ≥ 10y Remedial Operations: • PTA +/- stenting complicated remedial surgery in • – Aortic reimplantation (13), Semgental reimplantation (1), 56% of patients Aorto-renal bypass (10), Arterioplsty (1), Iliorenal bypass (1), Nephrectomy (7) No major morbidity, operative mortality or late • deaths Postoperative HTN cured (24%), improved • (60%), unchanged (16%) 8
4/6/2017 Indications for Endovascular Interventions 2017 Contemporary Update Endovascular therapy as a “bridge” to surgical • 218 children – 55% last decade • therapy –29% previous open or EV intervention prior to –Allowed delay of surgical reconstruction > 1 year transfer to UM 19% risk of reoperation • Small vessel size and fibrotic nature of stenoses –Age < 5 years at index surgery • limits endovascular utility 43% cure, 42% improvement, 14% • unchanged –Remedial operations and MAS – less likely to be Endovascular therapy for renal artery stenoses • cured of hypertension in pediatric patients should be undertaken with caution (high-volume center) UM Experience with Renal Artery 14yo, NF1, 2-drug HTN + FTT Aneurysms (N=15, 26 aneurysms) 3-25mm (avg 9mm) • 50% segmental • Coleman and Stanley; JVS; 2015 Treatment: • –Resection with primary anastomosis –Resection with reimplantation LRA resection, ex-vivo –Angioplastic closure reconstruction w/ –Nephrectomy (N=4) syndactylzation of 3 segmental branches, aorto- 15% reintervention Davis et al; JVS; 2016; 63.1 • renal bypass 9
4/6/2017 Conclusions Pediatric Vascular Surgery Team Open surgical revascularization may be • performed with negligible M&M Completion imaging and surveillance critical • Dawn Coleman MD Jon Eliason MD Multidisciplinary team important • James C Stanley MD Pediatric Vascular Program Thank You Pediatric Nephrology Vascular Surgery • • – David Kershaw – James Stanley – Neal Blatt – Jonathan Eliason – David Selewski – Dawn Coleman – Kera Luckritz Interventional Radiology • Pediatric Urology • – David Williams – John Park – Ravi Srinavasa PICU Nurse Coordinators • • – Char Minard Pediatric Anesthesia • – Susan Young Social Work • – Matt Butler 10
4/6/2017 Fibromuscular Dysplasia (FMD) Histopathological Classification Histologic (1971) Angiographic Non-atherosclerotic, non-inflammatory • Harrison and McCormack French/Belgian **AHA (2014) vascular disease that may result in arterial Consensus (2012) stenosis, occlusion, aneurysm or dissection Medial : Multifocal Multifocal (‘string of Medial fibroplasia (60-70%) beads’) Perimedial fibroplasia (15-25%) Medial hyperplasia (1-2%) Cause unknown Intimal fibroplasia (1-2) Unifocal (<1cm) Focal • Tubular ( ≥ 1cm) Prevalence unclear • Adventitial (<1%) Adapted from Olin et al, Circulation, 2014 Clinical manifestations dependent on Focal FMD: • Younger at diagnosis and onset of HTN (26 v 40y) vascular bed involved Male:Female (2:1) More likely to undergo revascularization (90 v 35%) Higher rate of HTN cure (54 v 26%) Savard et al, Circulation, 2012 Renal FMD Suspect FMD when: • –Early onset HTN (<35 years) –Medically-refractory HTN Average age of onset ~ 43.1 years • Renal insufficiency, dissection, infarction and • CKD uncommon Multifocal / Medial H/A common FMD • Olin et al, Circulation, 2014 11
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries