Reducing medical spending of the publicly insured: the case for - PowerPoint PPT Presentation
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Reducing medical spending of the publicly insured: the case for cash-out option Svetlana Pashchenko Ponpoje
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A This paper Constructs the model where: - Not all medical spending are necessary - Individuals choose discretionary medical spending given their insurance coverage - Insurance coverage is endogenous (selection) Studies how to improve public health insurance when: - Main friction: discretionary/necessary division of medical spending is unobservable - Beneficiaries have low income = > risk-exposure is costly for welfare Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A This paper Constructs the model where: - Not all medical spending are necessary - Individuals choose discretionary medical spending given their insurance coverage - Insurance coverage is endogenous (selection) Studies how to improve public health insurance when: - Main friction: discretionary/necessary division of medical spending is unobservable - Beneficiaries have low income = > risk-exposure is costly for welfare Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Approach Theoretical analysis: Mirrlesian framework: a planner observes total medical spending but not their composition (discretionary/non-discretionary) Use it to find optimal insurance policy Quantitative analysis: Rich structural life cycle model with heterogeneous agents Construct full information benchmark: discretionary medical spending is observable Assess policies based on how close they can get to the full information benchmark Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Approach Theoretical analysis: Mirrlesian framework: a planner observes total medical spending but not their composition (discretionary/non-discretionary) Use it to find optimal insurance policy Quantitative analysis: Rich structural life cycle model with heterogeneous agents Construct full information benchmark: discretionary medical spending is observable Assess policies based on how close they can get to the full information benchmark Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Approach Theoretical analysis: Mirrlesian framework: a planner observes total medical spending but not their composition (discretionary/non-discretionary) Use it to find optimal insurance policy Quantitative analysis: Rich structural life cycle model with heterogeneous agents Construct full information benchmark: discretionary medical spending is observable Assess policies based on how close they can get to the full information benchmark Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Approach Theoretical analysis: Mirrlesian framework: a planner observes total medical spending but not their composition (discretionary/non-discretionary) Use it to find optimal insurance policy Quantitative analysis: Rich structural life cycle model with heterogeneous agents Construct full information benchmark: discretionary medical spending is observable Assess policies based on how close they can get to the full information benchmark Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Approach Theoretical analysis: Mirrlesian framework: a planner observes total medical spending but not their composition (discretionary/non-discretionary) Use it to find optimal insurance policy Quantitative analysis: Rich structural life cycle model with heterogeneous agents Construct full information benchmark: discretionary medical spending is observable Assess policies based on how close they can get to the full information benchmark Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Approach Theoretical analysis: Mirrlesian framework: a planner observes total medical spending but not their composition (discretionary/non-discretionary) Use it to find optimal insurance policy Quantitative analysis: Rich structural life cycle model with heterogeneous agents Construct full information benchmark: discretionary medical spending is observable Assess policies based on how close they can get to the full information benchmark Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Approach Theoretical analysis: Mirrlesian framework: a planner observes total medical spending but not their composition (discretionary/non-discretionary) Use it to find optimal insurance policy Quantitative analysis: Rich structural life cycle model with heterogeneous agents Construct full information benchmark: discretionary medical spending is observable Assess policies based on how close they can get to the full information benchmark Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Theoretical analysis Individuals differ in their medical need: η L and η H , η L < η H Measure of L-type is π , measure of H-type is 1 − π Individuals derive utility from regular consumption u ( c ) discretionary medical consumption v ( m − η ), m > η Social planner maximizes social welfare by allocating resources B , B < η H Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Theoretical analysis Individuals differ in their medical need: η L and η H , η L < η H Measure of L-type is π , measure of H-type is 1 − π Individuals derive utility from regular consumption u ( c ) discretionary medical consumption v ( m − η ), m > η Social planner maximizes social welfare by allocating resources B , B < η H Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Theoretical analysis Individuals differ in their medical need: η L and η H , η L < η H Measure of L-type is π , measure of H-type is 1 − π Individuals derive utility from regular consumption u ( c ) discretionary medical consumption v ( m − η ), m > η Social planner maximizes social welfare by allocating resources B , B < η H Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Theoretical analysis Individuals differ in their medical need: η L and η H , η L < η H Measure of L-type is π , measure of H-type is 1 − π Individuals derive utility from regular consumption u ( c ) discretionary medical consumption v ( m − η ), m > η Social planner maximizes social welfare by allocating resources B , B < η H Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Medical need is private information Social planner’s problem: π [ u ( c L ) + v ( m L − η L )]+(1 − π ) [ u ( c H ) + v ( m H − η H )] − → max { c i , m i } i = L , H s.t. π [ c L + m L ] + (1 − π ) [ c H + m H ] = B Incentive compatibility constraint: u ( c L ) + v ( m L − η L ) ≥ u ( c H ) + v ( m H − η L ) Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Medical need is private information Social planner’s problem: π [ u ( c L ) + v ( m L − η L )]+(1 − π ) [ u ( c H ) + v ( m H − η H )] − → max { c i , m i } i = L , H s.t. π [ c L + m L ] + (1 − π ) [ c H + m H ] = B Incentive compatibility constraint: u ( c L ) + v ( m L − η L ) ≥ u ( c H ) + v ( m H − η L ) Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Medical need is private information Social planner’s problem: π [ u ( c L ) + v ( m L − η L )]+(1 − π ) [ u ( c H ) + v ( m H − η H )] − → max { c i , m i } i = L , H s.t. π [ c L + m L ] + (1 − π ) [ c H + m H ] = B Incentive compatibility constraint: u ( c L ) + v ( m L − η L ) ≥ u ( c H ) + v ( m H − η L ) Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Properties of the solution Individuals reporting low medical need get rewarded with higher regular consumption: c ∗ L > c ∗ H , m ∗ L < m ∗ H Consumption of individuals with low medical need should be undistorted: u ′ ( c ∗ L ) = v ′ ( m ∗ L − η L ) Consumption of individuals with high medical need should be distorted: u ′ ( c ∗ H ) > v ′ ( m ∗ H − η H ) Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Properties of the solution Individuals reporting low medical need get rewarded with higher regular consumption: c ∗ L > c ∗ H , m ∗ L < m ∗ H Consumption of individuals with low medical need should be undistorted: u ′ ( c ∗ L ) = v ′ ( m ∗ L − η L ) Consumption of individuals with high medical need should be distorted: u ′ ( c ∗ H ) > v ′ ( m ∗ H − η H ) Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Properties of the solution Individuals reporting low medical need get rewarded with higher regular consumption: c ∗ L > c ∗ H , m ∗ L < m ∗ H Consumption of individuals with low medical need should be undistorted: u ′ ( c ∗ L ) = v ′ ( m ∗ L − η L ) Consumption of individuals with high medical need should be distorted: u ′ ( c ∗ H ) > v ′ ( m ∗ H − η H ) Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Implementation The following transfer system implements the optimum. Individuals get a choice between two insurance plans Plan 1: - cash transfers T L Plan 2: - cash transfers T H ( T H < T L ) - health insurance that covers 1 − q of medical spending Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Implementation The following transfer system implements the optimum. Individuals get a choice between two insurance plans Plan 1: - cash transfers T L Plan 2: - cash transfers T H ( T H < T L ) - health insurance that covers 1 − q of medical spending Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Implementation The following transfer system implements the optimum. Individuals get a choice between two insurance plans Plan 1: - cash transfers T L Plan 2: - cash transfers T H ( T H < T L ) - health insurance that covers 1 − q of medical spending Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Implementation The following transfer system implements the optimum. Individuals get a choice between two insurance plans Plan 1: - cash transfers T L Plan 2: - cash transfers T H ( T H < T L ) - health insurance that covers 1 − q of medical spending Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Summary Optimal policy should create a trade-off between regular and medical consumption This can be implemented by allowing individuals to substitute health insurance with cash transfers Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Summary Optimal policy should create a trade-off between regular and medical consumption This can be implemented by allowing individuals to substitute health insurance with cash transfers Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Model: households Life-cycle model: 25-64 → work, 65-99 → retired Agents face productivity, health, medical need, and survival risks Two types of health insurance for working age households 1 Employer-sponsored insurance - ESI (if getting an offer) 2 Medicaid: income test asset test k t r + z h t l t < y cat and k t < k cat Eligibility: All retired households are insured by Medicare Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Model: households Life-cycle model: 25-64 → work, 65-99 → retired Agents face productivity, health, medical need, and survival risks Two types of health insurance for working age households 1 Employer-sponsored insurance - ESI (if getting an offer) 2 Medicaid: income test asset test k t r + z h t l t < y cat and k t < k cat Eligibility: All retired households are insured by Medicare Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Model: households Life-cycle model: 25-64 → work, 65-99 → retired Agents face productivity, health, medical need, and survival risks Two types of health insurance for working age households 1 Employer-sponsored insurance - ESI (if getting an offer) 2 Medicaid: income test asset test k t r + z h t l t < y cat and k t < k cat Eligibility: All retired households are insured by Medicare Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Model: households Life-cycle model: 25-64 → work, 65-99 → retired Agents face productivity, health, medical need, and survival risks Two types of health insurance for working age households 1 Employer-sponsored insurance - ESI (if getting an offer) 2 Medicaid: income test asset test k t r + z h t l t < y cat and k t < k cat Eligibility: All retired households are insured by Medicare Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Model: households Life-cycle model: 25-64 → work, 65-99 → retired Agents face productivity, health, medical need, and survival risks Two types of health insurance for working age households 1 Employer-sponsored insurance - ESI (if getting an offer) 2 Medicaid: income test asset test k t r + z h t l t < y cat and k t < k cat Eligibility: All retired households are insured by Medicare Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Model: households Life-cycle model: 25-64 → work, 65-99 → retired Agents face productivity, health, medical need, and survival risks Two types of health insurance for working age households 1 Employer-sponsored insurance - ESI (if getting an offer) 2 Medicaid: income test asset test k t r + z h t l t < y cat and k t < k cat Eligibility: All retired households are insured by Medicare Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Model: households (working ages) health condition ( h t ) medical need ( η h t ) labor productivity ( z h t ) Medicaid eligibility is determined ESI offer ( g h , z ) t t+1 t k t � � saving ( k t +1 ) labor supply: l t ∈ 0 , l insurance ( i H ) consumption ( c t ) - uninsured medical consumption ( m t ) - ESI Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Model: households (working ages) health condition ( h t ) medical need ( η h t ) labor productivity ( z h t ) Medicaid eligibility is determined ESI offer ( g h , z ) t t+1 t k t � � saving ( k t +1 ) labor supply: l t ∈ 0 , l insurance ( i H ) consumption ( c t ) - uninsured medical consumption ( m t ) - ESI Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Model: households (working ages) health condition ( h t ) medical need ( η h t ) labor productivity ( z h t ) Medicaid eligibility is determined ESI offer ( g h , z ) t t+1 t k t � � saving ( k t +1 ) labor supply: l t ∈ 0 , l insurance ( i H ) consumption ( c t ) - uninsured medical consumption ( m t ) - ESI Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Model: households (working ages) health condition ( h t ) medical need ( η h t ) labor productivity ( z h t ) Medicaid eligibility is determined ESI offer ( g h , z ) t t+1 t k t � � saving ( k t +1 ) labor supply: l t ∈ 0 , l insurance ( i H ) consumption ( c t ) - uninsured medical consumption ( m t ) - ESI Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Parametrization t ) 1 − σ M Utility from medical consumption: ( m t − η h 1 − σ M v ( m t , ∆) - quadratic function ∆ - saturation point Total medical spending is in the range ( η h t , η h t + ∆] Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Parametrization t ) 1 − σ M Utility from medical consumption: ( m t − η h 1 − σ M v ( m t , ∆) - quadratic function ∆ - saturation point Total medical spending is in the range ( η h t , η h t + ∆] Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Parametrization t ) 1 − σ M Utility from medical consumption: ( m t − η h + v ( m t , ∆) 1 − σ M v ( m t , ∆) - quadratic function ∆ - saturation point Total medical spending is in the range ( η h t , η h t + ∆] Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Parametrization t ) 1 − σ M Utility from medical consumption: ( m t − η h + v ( m t , ∆) 1 − σ M v ( m t , ∆) - quadratic function ∆ - saturation point Total medical spending is in the range ( η h t , η h t + ∆] Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Parametrization t ) 1 − σ M Utility from medical consumption: ( m t − η h + v ( m t , ∆) 1 − σ M v ( m t , ∆) - quadratic function ∆ - saturation point Total medical spending is in the range ( η h t , η h t + ∆] Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Parametrization t ) 1 − σ M Utility from medical consumption: ( m t − η h + v ( m t , ∆) 1 − σ M v ( m t , ∆) - quadratic function ∆ - saturation point Total medical spending is in the range ( η h t , η h t + ∆] CL Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
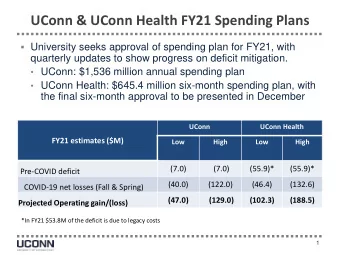
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Utility from medical consumption: illustration 0 −5 Medical need Saturation point −10 Utility −15 −20 −25 0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5 Medical spending Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Saturation point ∆ − > difference in medical expenses between privately insured and uninsured Total medical spending (fixed) = Non-discretionary spending + Discretionary spending ∆ ↑ ⇒ Discretionary spending ↑ ⇒ Non-discretionary spending ↓ ⇒ insured spend more compared to uninsured Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Saturation point ∆ − > difference in medical expenses between privately insured and uninsured Total medical spending (fixed) = Non-discretionary spending + Discretionary spending ∆ ↑ ⇒ Discretionary spending ↑ ⇒ Non-discretionary spending ↓ ⇒ insured spend more compared to uninsured Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Saturation point ∆ − > difference in medical expenses between privately insured and uninsured Total medical spending (fixed) = Non-discretionary spending + Discretionary spending ∆ ↑ ⇒ Discretionary spending ↑ ⇒ Non-discretionary spending ↓ ⇒ insured spend more compared to uninsured Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Medical need shock Medical need shock has shifted lognormal distribution η h t = exp( κ h t ) − exp( b h t ) b h t − > fraction of people with zero medical expenses κ h t = µ h t + δ h t ζ t , µ h t − > mean of medical expenses δ h t − > variance of medical expenses ζ t = ρ m ζ t − 1 + ε t , ε t ∼ N (0 , 1) LabInc ρ m − > persistence of medical expenses Param Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Medical need shock Medical need shock has shifted lognormal distribution η h t = exp( κ h t ) − exp( b h t ) b h t − > fraction of people with zero medical expenses κ h t = µ h t + δ h t ζ t , µ h t − > mean of medical expenses δ h t − > variance of medical expenses ζ t = ρ m ζ t − 1 + ε t , ε t ∼ N (0 , 1) LabInc ρ m − > persistence of medical expenses Param Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Medical need shock Medical need shock has shifted lognormal distribution η h t = exp( κ h t ) − exp( b h t ) b h t − > fraction of people with zero medical expenses κ h t = µ h t + δ h t ζ t , µ h t − > mean of medical expenses δ h t − > variance of medical expenses ζ t = ρ m ζ t − 1 + ε t , ε t ∼ N (0 , 1) LabInc ρ m − > persistence of medical expenses Param Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Medical need shock Medical need shock has shifted lognormal distribution η h t = exp( κ h t ) − exp( b h t ) b h t − > fraction of people with zero medical expenses κ h t = µ h t + δ h t ζ t , µ h t − > mean of medical expenses δ h t − > variance of medical expenses ζ t = ρ m ζ t − 1 + ε t , ε t ∼ N (0 , 1) LabInc ρ m − > persistence of medical expenses Param Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Insurance statistics 0.8 0.8 Medicaid, data Data ESHI, data Model 0.7 0.7 Medicaid, model % uninsured among healthy % insured among healthy ESHI, model 0.6 0.6 0.5 0.5 0.4 0.4 0.3 0.3 0.2 0.2 0.1 0.1 0 0 25−29 30−34 35−39 40−44 45−49 50−54 55−59 60−64 25−29 30−34 35−39 40−44 45−49 50−54 55−59 60−64 Age Age 0.8 0.8 Medicaid, data Data ESHI, data Model 0.7 0.7 % uninsured among unhealthy Medicaid, model % insured among unhealthy ESHI, model 0.6 0.6 0.5 0.5 0.4 0.4 0.3 0.3 0.2 0.2 0.1 0.1 0 0 25−29 30−34 35−39 40−44 45−49 50−54 55−59 60−64 25−29 30−34 35−39 40−44 45−49 50−54 55−59 60−64 Age Age Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Selection of unhealthy into Medicaid Data Baseline model ESHI uninsured public ESHI uninsured public % unhealthy by insurance 10.3 18.9 52.6 9.0 17.2 51.3 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Employment and labor income Average labor income profiles 1.2 1 0.8 0.6 0.4 Healthy, data 0.2 Healthy, model Unhealthy, data Unhealthy, model 0 25−29 30−34 35−39 40−44 45−49 50−54 55−59 60−64 Age 1 1 0.9 0.9 0.8 0.8 0.7 0.7 % employed % employed 0.6 0.6 0.5 0.5 0.4 0.4 0.3 0.3 ESI, data Uninsured, data 0.2 Healthy, data 0.2 Medicaid, data Healthy, model ESI, model 0.1 Unhealthy, data 0.1 Uninsured, model Unhealthy, model Medicaid, model 0 0 25−29 30−34 35−39 40−44 45−49 50−54 55−59 60−64 25−29 30−34 35−39 40−44 45−49 50−54 55−59 60−64 Age Age Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Medical expenses by health statistics 0.4 0.4 Healthy, data Healthy, data Healthy, model Healthy, model 0.35 0.35 Unhealthy, data Unhealthy, data Median of medical expenses Mean of medical expenses Unhealthy, model Unhealthy, model 0.3 0.3 0.25 0.25 0.2 0.2 0.15 0.15 0.1 0.1 0.05 0.05 0 0 25−29 35−39 45−49 55−59 65−69 75−79 85+ 25−29 35−39 45−49 55−59 65−69 75−79 85+ Age Age 0.5 0.4 Healthy, data Healthy, data 0.45 Healthy, model Healthy, model 0.35 % with zero medical expenses Unhealthy, data Unhealthy, data Unhealthy, model Unhealthy, model SD of medical expenses 0.4 0.3 0.35 0.25 0.3 0.25 0.2 0.2 0.15 0.15 0.1 0.1 0.05 0.05 0 0 25−29 35−39 45−49 55−59 65−69 75−79 85+ 25−29 35−39 45−49 55−59 65−69 75−79 85+ Age Age Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Medical expenses by insurance Uninsured, data ESI, data 0.3 Medicaid, data Mean of medical expenses Uninsured, model ESI, model 0.25 Medicaid, model 0.2 0.15 0.1 0.05 0 25−29 30−34 35−39 40−44 45−49 50−54 55−59 60−64 Age Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A The role of the saturation point Total medical expenses by insurance, baseline Uninsured ESI Medicaid 0.25 Mean of medical expenses 0.2 0.15 0.1 0.05 0 25−29 30−34 35−39 40−44 45−49 50−54 55−59 60−64 Age Total medical expenses by insurance, low saturation point Total medical expenses by insurance, high saturation point Uninsured Uninsured ESI ESI Medicaid Medicaid 0.25 0.25 Mean of medical expenses Mean of medical expenses 0.2 0.2 0.15 0.15 0.1 0.1 0.05 0.05 0 0 25−29 30−34 35−39 40−44 45−49 50−54 55−59 60−64 25−29 30−34 35−39 40−44 45−49 50−54 55−59 60−64 Age Age Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Full information benchmark Assume medical need η h t is observable The government (fully) covers non-discretionary medical spending The rest of welfare budget is allocated ass lump-sum transfers to Medicaid beneficiaries Thus individuals face full price of their discretionary medical consumption Consider one-time policy change: medical need is observable for only one period Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Full information benchmark, one time policy change Med spending Lump sum (% BS) transfers ($000) Baseline 100 - Observable need 94.1 5.3 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Full information benchmark, one time policy change Change in the life-cycle profile of medical spending of Medicaid enrollees: Mean of medical expenses of Medicaid beneficiaries 0.25 0.2 0.15 0.1 0.05 Baseline Observable medical need 0 25−29 30−34 35−39 40−44 45−49 50−54 55−59 60−64 Age Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Medical need is private information To fix the distribution of beneficiaries and illustrate the mechanism, consider first one-time policy change Start by using cost-sharing as the only instrument to decrease medical spending Consider gradual decrease in Medicaid generosity The saved budget is allocated as lump-sum cash transfers so that welfare budget is unchanged Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Increasing cost-sharing, one-time policy change Med spending Lump sum (% BS) transfers ($000) Baseline 100 - 1. Observable need 94.4 5.3 Increasing MCD copay 2. Medicaid covers 85% 98.5 1.8 3. Medicaid covers 80% 98.0 2.5 4. Medicaid covers 75% 97.4 2.9 5. Medicaid covers 70% 97.0 3.3 6. Medicaid covers 60% 96.2 3.9 7. Medicaid covers 50% 95.6 4.4 8. Medicaid covers 40% 95.1 4.9 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Increasing cost-sharing, one-time policy change Med spending Lump sum (% BS) transfers ($000) Baseline 100 - 1. Observable need 94.4 5.3 Increasing MCD copay 2. Medicaid covers 85% 98.5 1.8 3. Medicaid covers 80% 98.0 2.5 4. Medicaid covers 75% 97.4 2.9 5. Medicaid covers 70% 97.0 3.3 6. Medicaid covers 60% 96.2 3.9 7. Medicaid covers 50% 95.6 4.4 8. Medicaid covers 40% 95.1 4.9 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Increasing cost-sharing, one-time policy change Med spending Lump sum (% BS) transfers ($000) Baseline 100 - 1. Observable need 94.4 5.3 Increasing MCD copay 2. Medicaid covers 85% 98.5 1.8 3. Medicaid covers 80% 98.0 2.5 4. Medicaid covers 75% 97.4 2.9 5. Medicaid covers 70% 97.0 3.3 6. Medicaid covers 60% 96.2 3.9 7. Medicaid covers 50% 95.6 4.4 8. Medicaid covers 40% 95.1 4.9 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Increasing cost-sharing, one-time policy change Med spending Lump sum (% BS) transfers ($000) Baseline 100 - 1. Observable need 94.4 5.3 Increasing MCD copay 2. Medicaid covers 85% 98.5 1.8 3. Medicaid covers 80% 98.0 2.5 4. Medicaid covers 75% 97.4 2.9 5. Medicaid covers 70% 97.0 3.3 6. Medicaid covers 60% 96.2 3.9 7. Medicaid covers 50% 95.6 4.4 8. Medicaid covers 40% 95.1 4.9 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Increasing cost-sharing, one-time policy change Med spending Lump sum (% BS) transfers ($000) Baseline 100 - 1. Observable need 94.4 5.3 Increasing MCD copay 2. Medicaid covers 85% 98.5 1.8 3. Medicaid covers 80% 98.0 2.5 4. Medicaid covers 75% 97.4 2.9 5. Medicaid covers 70% 97.0 3.3 6. Medicaid covers 60% 96.2 3.9 7. Medicaid covers 50% 95.6 4.4 8. Medicaid covers 40% 95.1 4.9 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Increasing cost-sharing, one-time policy change Med spending Lump sum (% BS) transfers ($000) Baseline 100 - 1. Observable need 94.4 5.3 Increasing MCD copay 2. Medicaid covers 85% 98.5 1.8 3. Medicaid covers 80% 98.0 2.5 4. Medicaid covers 75% 97.4 2.9 5. Medicaid covers 70% 97.0 3.3 6. Medicaid covers 60% 96.2 3.9 7. Medicaid covers 50% 95.6 4.4 8. Medicaid covers 40% 95.1 4.9 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Increasing cost-sharing, one-time policy change Med spending Lump sum (% BS) transfers ($000) Baseline 100 - 1. Observable need 94.4 5.3 Increasing MCD copay 2. Medicaid covers 85% 98.5 1.8 3. Medicaid covers 80% 98.0 2.5 4. Medicaid covers 75% 97.4 2.9 5. Medicaid covers 70% 97.0 3.3 6. Medicaid covers 60% 96.2 3.9 7. Medicaid covers 50% 95.6 4.4 8. Medicaid covers 40% 95.1 4.9 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Increasing cost-sharing, one-time policy change Med spending Lump sum (% BS) transfers ($000) Baseline 100 - 1. Observable need 94.4 5.3 Increasing MCD copay 2. Medicaid covers 85% 98.5 1.8 3. Medicaid covers 80% 98.0 2.5 4. Medicaid covers 75% 97.4 2.9 5. Medicaid covers 70% 97.0 3.3 6. Medicaid covers 60% 96.2 3.9 7. Medicaid covers 50% 95.6 4.4 8. Medicaid covers 40% 95.1 4.9 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Increasing deductibles, one-time policy change Med spending Lump sum (% BS) transfers ($000) Baseline 100 - 1. Observable need 94.4 5.3 Increasing MCD deductibles 2. Deductibles 1K 99.4 1.5 3. Deductibles 2K 98.4 2.1 4. Deductibles 3K 97.7 2.7 5. Deductibles 5K 96.9 3.6 6. Deductibles 7K 96.4 4.4 7. Deductibles 10K 95.7 5.5 8. Deductibles 14K 95.2 6.4 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Increasing deductibles, one-time policy change Med spending Lump sum (% BS) transfers ($000) Baseline 100 - 1. Observable need 94.4 5.3 Increasing MCD deductibles 2. Deductibles 1K 99.4 1.5 3. Deductibles 2K 98.4 2.1 4. Deductibles 3K 97.7 2.7 5. Deductibles 5K 96.9 3.6 6. Deductibles 7K 96.4 4.4 7. Deductibles 10K 95.7 5.5 8. Deductibles 14K 95.2 6.4 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Increasing deductibles, one-time policy change Med spending Lump sum (% BS) transfers ($000) Baseline 100 - 1. Observable need 94.4 5.3 Increasing MCD deductibles 2. Deductibles 1K 99.4 1.5 3. Deductibles 2K 98.4 2.1 4. Deductibles 3K 97.7 2.7 5. Deductibles 5K 96.9 3.6 6. Deductibles 7K 96.4 4.4 7. Deductibles 10K 95.7 5.5 8. Deductibles 14K 95.2 6.4 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Increasing deductibles, one-time policy change Med spending Lump sum (% BS) transfers ($000) Baseline 100 - 1. Observable need 94.4 5.3 Increasing MCD deductibles 2. Deductibles 1K 99.4 1.5 3. Deductibles 2K 98.4 2.1 4. Deductibles 3K 97.7 2.7 5. Deductibles 5K 96.9 3.6 6. Deductibles 7K 96.4 4.4 7. Deductibles 10K 95.7 5.5 8. Deductibles 14K 95.2 6.4 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Increasing deductibles, one-time policy change Med spending Lump sum (% BS) transfers ($000) Baseline 100 - 1. Observable need 94.4 5.3 Increasing MCD deductibles 2. Deductibles 1K 99.4 1.5 3. Deductibles 2K 98.4 2.1 4. Deductibles 3K 97.7 2.7 5. Deductibles 5K 96.9 3.6 6. Deductibles 7K 96.4 4.4 7. Deductibles 10K 95.7 5.5 8. Deductibles 14K 95.2 6.4 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Increasing deductibles, one-time policy change Med spending Lump sum (% BS) transfers ($000) Baseline 100 - 1. Observable need 94.4 5.3 Increasing MCD deductibles 2. Deductibles 1K 99.4 1.5 3. Deductibles 2K 98.4 2.1 4. Deductibles 3K 97.7 2.7 5. Deductibles 5K 96.9 3.6 6. Deductibles 7K 96.4 4.4 7. Deductibles 10K 95.7 5.5 8. Deductibles 14K 95.2 6.4 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Increasing deductibles, one-time policy change Med spending Lump sum (% BS) transfers ($000) Baseline 100 - 1. Observable need 94.4 5.3 Increasing MCD deductibles 2. Deductibles 1K 99.4 1.5 3. Deductibles 2K 98.4 2.1 4. Deductibles 3K 97.7 2.7 5. Deductibles 5K 96.9 3.6 6. Deductibles 7K 96.4 4.4 7. Deductibles 10K 95.7 5.5 8. Deductibles 14K 95.2 6.4 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Increasing deductibles, one-time policy change Med spending Lump sum (% BS) transfers ($000) Baseline 100 - 1. Observable need 94.4 5.3 Increasing MCD deductibles 2. Deductibles 1K 99.4 1.5 3. Deductibles 2K 98.4 2.1 4. Deductibles 3K 97.7 2.7 5. Deductibles 5K 96.9 3.6 6. Deductibles 7K 96.4 4.4 7. Deductibles 10K 95.7 5.5 8. Deductibles 14K 95.2 6.4 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Introducing cash-out option Based on our theoretical analysis: cash-out option A choice between regular Medicaid benefits and lump-sum cash transfers Induces self-selection of individuals with low medical need into cash plan The size of the transfers is adjusted so the welfare budget is unchanged One-time policy change Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Introducing cash-out option Based on our theoretical analysis: cash-out option A choice between regular Medicaid benefits and lump-sum cash transfers Induces self-selection of individuals with low medical need into cash plan The size of the transfers is adjusted so the welfare budget is unchanged One-time policy change Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Introducing cash-out option Based on our theoretical analysis: cash-out option A choice between regular Medicaid benefits and lump-sum cash transfers Induces self-selection of individuals with low medical need into cash plan The size of the transfers is adjusted so the welfare budget is unchanged One-time policy change Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Introducing cash-out option Based on our theoretical analysis: cash-out option A choice between regular Medicaid benefits and lump-sum cash transfers Induces self-selection of individuals with low medical need into cash plan The size of the transfers is adjusted so the welfare budget is unchanged One-time policy change Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Introducing cash-out option Based on our theoretical analysis: cash-out option A choice between regular Medicaid benefits and lump-sum cash transfers Induces self-selection of individuals with low medical need into cash plan The size of the transfers is adjusted so the welfare budget is unchanged One-time policy change Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Introducing cash-out option Based on our theoretical analysis: cash-out option A choice between regular Medicaid benefits and lump-sum cash transfers Induces self-selection of individuals with low medical need into cash plan The size of the transfers is adjusted so the welfare budget is unchanged One-time policy change Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Results of introducing cash-out option: one-time policy change Med Lump sum % in cash spending transfers plan (% BS) ($000) ages 25-64 Baseline 100 - - 1. Observable need 94.4 5.3 - Increasing MCD copay 2. BS (93%) 99.0 1.6 65-24 3. Medicaid covers 85% 96.3 3.9 74-71 4. Medicaid covers 80% 95.8 4.5 79-76 5. Medicaid covers 75% 95.3 4.9 86-76 6. Medicaid covers 70% 95.1 5.4 90-76 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Results of introducing cash-out option: one-time policy change Med Lump sum % in cash spending transfers plan (% BS) ($000) ages 25-64 Baseline 100 - - 1. Observable need 94.4 5.3 - Increasing MCD copay 2. BS (93%) 99.0 1.6 65-24 3. Medicaid covers 85% 96.3 3.9 74-71 4. Medicaid covers 80% 95.8 4.5 79-76 5. Medicaid covers 75% 95.3 4.9 86-76 6. Medicaid covers 70% 95.1 5.4 90-76 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Results of introducing cash-out option: one-time policy change Med Lump sum % in cash spending transfers plan (% BS) ($000) ages 25-64 Baseline 100 - - 1. Observable need 94.4 5.3 - Increasing MCD copay 2. BS (93%) 99.0 1.6 65-24 3. Medicaid covers 85% 96.3 3.9 74-71 4. Medicaid covers 80% 95.8 4.5 79-76 5. Medicaid covers 75% 95.3 4.9 86-76 6. Medicaid covers 70% 95.1 5.4 90-76 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Introduction Theoretical analysis Quantitative model Calibration Model performance Results Improving target efficiency A Results of introducing cash-out option: one-time policy change Med Lump sum % in cash spending transfers plan (% BS) ($000) ages 25-64 Baseline 100 - - 1. Observable need 94.4 5.3 - Increasing MCD copay 2. BS (93%) 99.0 1.6 65-24 3. Medicaid covers 85% 96.3 3.9 74-71 4. Medicaid covers 80% 95.8 4.5 79-76 5. Medicaid covers 75% 95.3 4.9 86-76 6. Medicaid covers 70% 95.1 5.4 90-76 Svetlana Pashchenko and Ponpoje Porapakkarm Reducing medical spending of the publicly insured: the case for
Recommend







![I mplemented Systems Logical Agents Reasoning [Ch 6] Propositional Logic [Ch 7]](https://c.sambuz.com/767929/i-mplemented-systems-logical-agents-s.webp)
More recommend
Explore More Topics
Stay informed with curated content and fresh updates.