RAPID VERSUS SLOW REWARMING FOR MANAGEMENT OF MODERATE TO SEVERE - PowerPoint PPT Presentation
RAPID VERSUS SLOW REWARMING FOR MANAGEMENT OF MODERATE TO SEVERE HYPOTHERMIA IN LOW BIRTH WEIGHT PRETERM NEONATES - A RANDOMIZED CONTROLLED TRIAL Dr Prerana Jain, MD Pediatrics, Department of Pediatrics Pt B D Sharma Post Graduate Institute of
RAPID VERSUS SLOW REWARMING FOR MANAGEMENT OF MODERATE TO SEVERE HYPOTHERMIA IN LOW BIRTH WEIGHT PRETERM NEONATES - A RANDOMIZED CONTROLLED TRIAL Dr Prerana Jain, MD Pediatrics, Department of Pediatrics Pt B D Sharma Post Graduate Institute of Medical Sciences, Rohtak Dr Jagjit Dalal, Associate Professor, Department of Pediatrics And Neonatology Pt B D Sharma Post Graduate Institute of Medical Sciences, Rohtak
INTRODUCTION ■ Temperature loss in a newborn will result in neonatal hypothermia with serious and potentially fatal consequences if not prevented or managed appropriately. 1 ■ Rewarming is a key step to prevent life threatening morbidities and mortality in hypothermic neonates. ■ But evidence is lacking regarding optimal method for attaining normothermia, whether rapid rewarming or slow rewarming should be done. ■ The traditional recommendation has been that slow rewarming is preferable to rapid rewarming to avoid complications such as apnea and arrhythmias. 2-5 Other studies 2,6-9 have shown that a combination of neonatal intensive care plus rapid rewarming ■ under a radiant warmer resulted in minimal mortality.
■ There is no direct study available for which mode to prefer between slow and rapid rewarming in moderate to severe hypothermia cases, specially in low resource countries like India where servo control radiant warmers are also not widely available. ■ So we planned a study to evaluate the effect of rapid versus slow rewarming in management of moderate to severe hypothermia in LBW preterm neonates in our hospital’s emergency setting.
AIM AND OBJECTIVES ■ Aim The aim of the study was to evaluate the effect of rapid versus slow rewarming in management of moderate to severe hypothermia in LBW preterm neonates. ■ Objectives of study: 1. Primary objective: Compare the effect of rapid versus slow rewarming in moderate - severely hypothermic low birth weight preterm neonates as assessed by stabilization score at baseline, 6 hours and 24 hours of enrollment. [TOPS (temperature, oxygenation, perfusion, saturation) and MSNS (modified sick neonatal score) scores] and mortality at 24 hours of enrolment and during hospital stay till discharge or death. 2. Secondary objective: Compare the proportion of neonates developing morbidities like sepsis, NEC (necrotizing enterocolitis), IVH (intraventricular hemorrhage), RDS (respiratory distress), hypoglycemia, apnea, need for intubation or respiratory support; time to reach normal body temperature (normothermia) and rewarming rate between the two groups.
MATERIAL AND METHODS ■ The study was done in the Department of Pediatrics, PGIMS Rohtak from September 2017 to December 2018. Ethical clearance was obtained from the Institutional Board of Studies. A pre informed consent was obtained from either of the parents. ■ Type of study: Randomized controlled trial, open label. ■ A total of 100 low birth weight preterm neonates weighing <2.5kg and gestation <37week with axillary/ skin temperature of <36 o C presenting within the first 72 hours of life were included in the study and randomized into two groups by computer generated random sequence numbers; group A received rapid rewarming (@ >0.5 o C/hr ) and group B received slow rewarming (@ ≤ 0.5 o C/hr) after attaining 34 o C, till normothermia (36.5 o C) is achieved by the neonates.
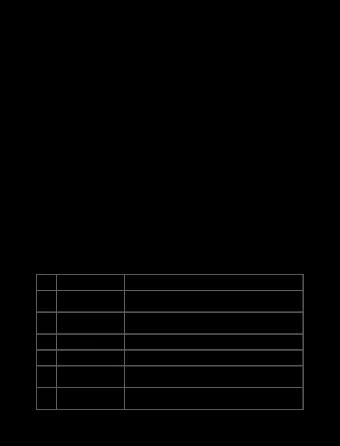
Moderate to severe • Preterm neonates with <1 Kg hypothermia (<36 o C) weight • Neonates with GCMF • Neonatal death before normothermia Assessed for • Parents/legally acceptable eligibility representative (LAR) not Exclusion criteria giving consent to participate • Neonates with refractory shock Randomised Group B Undergo slow rewarming (≤0.5 o C/hr) If temperature <34 o C: rewarming a) Group A under radiant warmer till 34 o C; after that slow rewarming at Undergo rapid rewarming (>0.5 o C/hr) @0.5 o C/hr till 36.5 o C skin under radiant warmer in servo control temperature (5hr) mode till the skin temperature reaches b) If temperature is between 34- 36.5 o C . 35.9 o C: keep directly under servo control mode for slow rewarming Continous HR, RR, at 0.5 o C/hr SpO2, temperature monitored Secondary Secondary Primary outcome Primary outcome outcome outcome Compared and evaluated Figure 1 Diagram showing the flow of patients
■ Sample Size: A sample size of 50 in each group over a period of 1 year was taken. The sample size was calculated using Epilnfo software. ■ Statistical Analysis: Data obtained was analysed by statistically standard tests. Statistical testing was conducted with the statistical package for the social science system version SPSS 17.0.
TOPS (Temperature, oxygenation, Perfusion and Sugar) score ■ TOPS includes: a. Temperature by digital thermometer in axilla or skin b. Oxygenation by SpO 2 monitoring (pulse oximeter) c. Perfusion by capillary refilling time (CFT) on mid-sternum Sugar by reagent strip and low reading glucometer <40mg/dl. 10 d. ■ Hypothermia, hypoxia, prolonged CFT and hypoglycaemia were defined as <36.5 ° C 11 , <90% 12 , ≥ 3 seconds 13 and < 40 mg/dl, respectively. ■ All the four parameters were assessed at baseline, 6 hours and 24 hours post admission of each subject and TOPS score was calculated along with the change in TOPS score since admission.
MSNS (Modified Sick Neonatal Score) score. Parameter Score 0 Score 1 Score 2 Tachypnoea Normal (respiratory rate (respiratory rate 40 – 60/min) Respiratory Apnoea or grunt >60/min) with or ■ MSNS score is essentially a modification of effort without retractions another validated scoring system, Sick Neonate Normal (100 – Heart rate Bradycardia or Tachycardia Score and studied among transported neonates. asystole (>160/min) 160/min) 36 – 36.5 36.5 – 37.5 Axillary <36 temperature ■ It has 8 parameters, each given a score of 0 to ( ° C) Capillary >5 3-5 <3 refilling time (s) 2. Score 0 implied the worst, and score 2 Random blood <40 40-60 >60 implied the best possible clinical setting for sugar (mg/dl) Maximum Spo2 <85 85-92 >92 each of the parameters. 14 (%) Gestational age <32 weeks 32 to 36 weeks + 37 weeks and (in weeks) 6/7 days above Birth weight <1.5 1.5-2.49 2.5 or above (kg) Total Maximum 16 Table I Parameters of MSNS with scoring for each parameter 14
RESULTS 267 neonates presented in casualty over 1 year 74 neonates excluded with no/mild hypothermia 193 neonates with moderate-severe hypothermia In our study, total 267 neonates presented in casualty over a period of 1 year. Out of Accessed for them, 100 neonates were included in the eligibility 100 neonates 74 neonates included excluded study (Figure 2). 100/119 neonates included • Preterm neonates with Low birth weight <1 Kg weight (22) • neonates <2.5 kg Neonates with GCMF (17) Gestation <37 week 100 neonates • Neonatal death before Presenting within 72 normothermia (0) Randomised • Parents/legally hours of life acceptable representative (LAR) not giving consent to participate (3) • Figure 2 Algorithm showing inclusion of patients Neonates with 50 neonates 50 neonates refractory shock (32) Group A Group B Rapid rewarming Slow rewarming
■ All the foetal and maternal baseline characteristics were equally distributed amongst the two groups and statistically not significant. ■ Statistically significant difference was found in the rewarming rates and rewarming time between the two groups. The mean rewarming rate in group A was 0.11 ± 0.07 ( o C/min), while in group B it was 0.012 ± 0.002 ( o C/min) (p value <0.001), with calculated odds ratio being 0.097 (0.07- 0.12). ■ Mean rewarming time taken in rapid rewarming group was 28.72 ± 28.90 min and in slow rewarming group was 157.78 ± 107 min. p value calculated was <0.001 (statistically significant). ■ Primary outcome was assessed by stabilization score (TOPS and MSNS score) and mortality at 24 hours of enrolment and during hospital stay till discharge or death . ■ TOPS score was used at baseline, 6 hours and 24 hours post admission to assess the stabilization of neonates. Results were not significant.
Mean MSNS score in rapid rewarming group was 9.92 ± 1.91 and in slow rewarming group was 10.14 ± 1.93, with a p value of 0.569 (95% CI = 9.37 - 10.46). The results were also statistically not significant at 6 hours and 24 hours post admission, between the two groups. (p value= 0.476 and 0.333, respectively) as described in Table II. MSNS Score Rapid rewarming Slow rewarming p- value (mean ± SD) (mean ± SD) 9.92 ± 1.91 10.14 ± 1.93 MSNS score at 0.569 admission 12.18 ± 1.88 12.06 ± 1.85 MSNS score at 0.476 6 hours 12.08 ± 1.72 12.12 ± 1.69 MSNS score at 0.333 24 hours Table II Stabilization assessed as per MSNS score at admission, 6 hours and 24 hours after admission
Total mortality in group A was 7 (14%) and in group B was 5 (10%). (p value=0.538). There is also no significant difference in mortality between the two groups when calculated within 24 hours and more than 24 hours of hospital stay. (Table III) Rapid rewarming Slow rewarming Mortality OR p value (n=50) (n=50) (95% CI) n (%) n (%) Total mortality 7 (14.0) 5 (10.0) 1.46 (0.43-4.97) 0.538 Mortality within 4 (8.0)1 1 (2.0) 4 (0.21-75.65) 0.343 24 hours Mortality >24 hours 3 (6.0) 4 (8.0) 0.78 (0.16-3.73) 0.762 Table III Mortality in rapid and slow rewarming group
Recommend





More recommend
Explore More Topics
Stay informed with curated content and fresh updates.