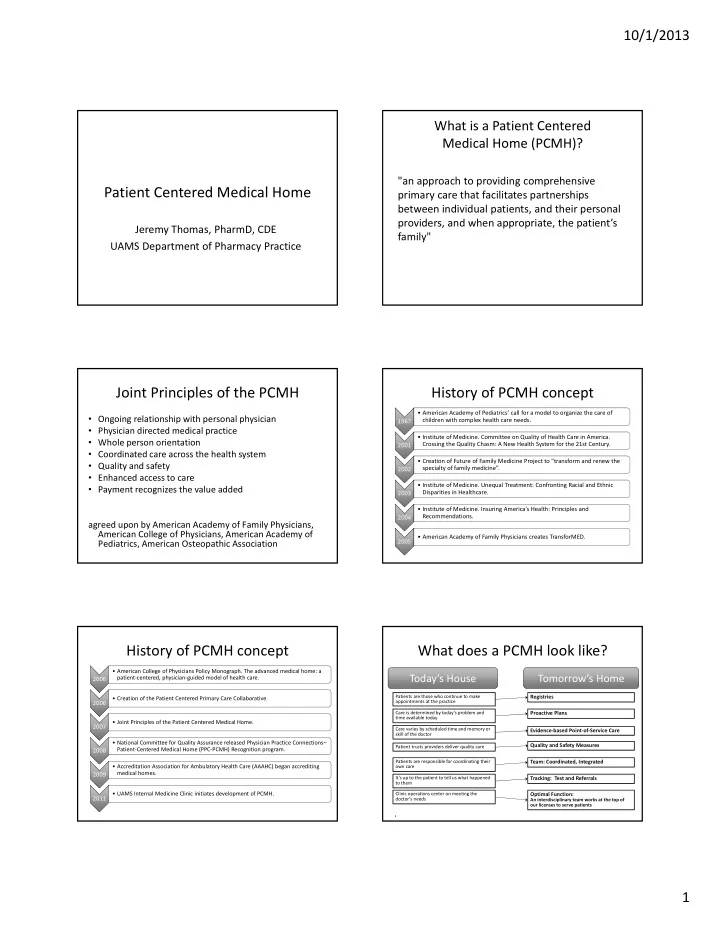
10/1/2013 What is a Patient Centered Medical Home (PCMH)? "an approach to providing comprehensive Patient Centered Medical Home primary care that facilitates partnerships between individual patients, and their personal providers, and when appropriate, the patient’s Jeremy Thomas, PharmD, CDE family" UAMS Department of Pharmacy Practice Joint Principles of the PCMH History of PCMH concept • American Academy of Pediatrics’ call for a model to organize the care of • Ongoing relationship with personal physician children with complex health care needs. 1967 1967 • Physician directed medical practice • Institute of Medicine. Committee on Quality of Health Care in America. • Whole person orientation Crossing the Quality Chasm: A New Health System for the 21st Century. 2001 2001 • Coordinated care across the health system • Creation of Future of Family Medicine Project to "transform and renew the • Quality and safety specialty of family medicine”. 2002 2002 • Enhanced access to care • Institute of Medicine. Unequal Treatment: Confronting Racial and Ethnic • Payment recognizes the value added Disparities in Healthcare. 2003 2003 • Institute of Medicine. Insuring America’s Health: Principles and Recommendations. 2004 2004 agreed upon by American Academy of Family Physicians, American College of Physicians, American Academy of • American Academy of Family Physicians creates TransforMED. 2005 2005 Pediatrics, American Osteopathic Association History of PCMH concept What does a PCMH look like? • American College of Physicians Policy Monograph. The advanced medical home: a Today’s House Tomorrow’s Home patient ‐ centered, physician ‐ guided model of health care. 2006 2006 Patients are those who continue to make Registries • Creation of the Patient Centered Primary Care Collaborative. appointments at the practice 2006 2006 Care is determined by today’s problem and Proactive Plans time available today • Joint Principles of the Patient Centered Medical Home. 2007 2007 Care varies by scheduled time and memory or Evidence ‐ based Point ‐ of ‐ Service Care skill of the doctor • National Committee for Quality Assurance released Physician Practice Connections– Quality and Safety Measures Patient trusts providers deliver quality care Patient ‐ Centered Medical Home (PPC ‐ PCMH) Recognition program. 2008 2008 Patients are responsible for coordinating their Team: Coordinated, Integrated • Accreditation Association for Ambulatory Health Care (AAAHC) began accrediting own care medical homes. 2009 2009 It’s up to the patient to tell us what happened Tracking: Test and Referrals to them 2011 • UAMS Internal Medicine Clinic initiates development of PCMH. Clinic operations center on meeting the Optimal Function: 2011 doctor’s needs An interdisciplinary team works at the top of our licenses to serve patients 6 1
10/1/2013 Business & Clinical Connectivity & Evidence ‐ Based Clinical Data Analysis Building Blocks of a PCMH Process Automation Communication Medicine Support & Representation • Evidence ‐ based • All patient, all condition • Intra ‐ office team • E ‐ prescribing template for registry coordination documentation • Clinical messaging • Quality measurement • Results, referrals and • Access to online with patients collection and analysis procedures tracking medical information • Health information • Reporting to third • Schedule and resource • Clinical decision parties exchange Great management support Outcomes Quality Patient Measures Experience Health Heath Practice Information Information Organization Technology Technology Patient Centeredness Patient Centeredness Financial Management Personnel Management Clinical Systems Culture of Performance Reliable Improvement Measurement Systems • Lab testing • Every team member • All staff are aware of the • Quality measures should • Prescriptions understands the important • Staff education • Develop reliable systems most effective ways to • Registries role they play in delivering be based in clinical deliver care • Lab testing • Team meetings to collect information efficient care and is evidence • National policies support the • Prescriptions empowered to make • Ensure quality • Check list and reminders investment of resources into • Patient Registries • Patient satisfaction suggestions for improvement initiatives • Evidence ‐ based decision primary care practices that surveys improvement are effective and efficient are not punitive support tool Quality Measures Health Patient Health Practice Practice Information Experience Information Organization Organization Technology Technology Patient Centeredness Patient Centeredness Convenient Access Personalized Care Care Coordination Great Outcomes • Reminders • Referral management • Good for patients • Same ‐ day appointments • Non ‐ physician care • Patent engagement and • After ‐ hours access – Patients enjoy better health. management education coverage • Shared decision ‐ making • Prevention screening and – Patients share in health care decisions. • Online patient services • Self ‐ management support services Great • Good for physicians Outcomes – Physicians focus on delivering excellent Patient medical care. Quality Health Experience Measures Quality Patient Information • Good for practices Measures Technology Experience – Team works effectively together. Patient – Resources support the delivery of excellent Experience Heath Practice Health Practice patient care. Information Organization Information Organization Technology Technology • Good for payors and employers Family Medicine Foundation Patient Centeredness – Ensures quality and efficiency. Patient Centeredness – Avoids unnecessary costs. 2
10/1/2013 Outcomes of PCMH Interventions Outcomes of PCMH Interventions Group Health Cooperative of Puget Sound Geisinger Health System • 29% reduction in ER visits and 11% reduction in • Statistically significant improvements in quality of ambulatory sensitive care admission preventive (74.0% improvement), coronary artery disease (22.0%) and diabetes care (34.5%) for PCMH Community Care of North Carolina pilot practice sites 93% of asthmatics received appropriate maintenance • medications Genesee Health Plan 40% decrease in hospitalizations for asthma and 16% lower ER • visit rate • 72% of the uninsured adults in Genesee County now identify a primary care practice as their Health Partners Medical Group MN medical home • 350% reduction in appointment waiting time The Outcomes of Implementing Patient ‐ Centered Medical Home Interventions: A Review of the Evidence on Quality, Access and Costs The Outcomes of Implementing Patient ‐ Centered Medical Home Interventions: A Review of the Evidence on Quality, Access and Costs from Recent Prospective Evaluation Studies, August 2009. www.pcpcc.net from Recent Prospective Evaluation Studies, August 2009. www.pcpcc.net Outcomes of PCMH Interventions Intermountain Healthcare Medical Group Management Plus • 39% Decrease in emergency room admissions • 24% Decrease in hospital admissions • Net reduction cost of $640 per patient and $1,650 among high risk patients The Patient Centered Medical Home Blue Cross Blue Shield of NC ‐ Palmetto PHARMACIST INVOLVEMENT Primary Care Physicians • 12.4% decrease in ER visits • 10% decrease in hospital admissions • Total medical and pharmacy costs were 6.5% lower The Outcomes of Implementing Patient ‐ Centered Medical Home Interventions: A Review of the Evidence on Quality, Access and Costs from Recent Prospective Evaluation Studies, August 2009. www.pcpcc.net Identify and Manage Patient Populations NCQA PCMH 2011 Standards Standard 2, Element B • Enhance Access and Continuity Practice uses a searchable electronic system to • Identify and Manage Patient Populations record the following data: • Plan and Manage Care • Allergies, including medication allergies and • Provide Self ‐ Care Support and Community adverse reactions, for more than 80% of Resources patients • Track and Coordinate Care • List of prescription medications with the date • Measure and Improve Performance of updates for more than 80% of patients 3
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries