6/7/2018 N O F I N A N C I A L D I S C LO S U R E S PAT I E N T W. N . What testing options should be offered? • 37-year-old G5P4004 at 12 57% weeks gestation A. Cell free DNA -3 healthy children -1 son with Wolf-Hirschorn 33% B. Invasive testing with CVS syndrome C. Cell free DNA with CVS only if abnormal - Parental testing performed 11% Father is a carrier of a • balanced translocation Cell free DNA Invasive testing with CVS Cell free DNA with CVS only .. ** 25% recurrence risk 1
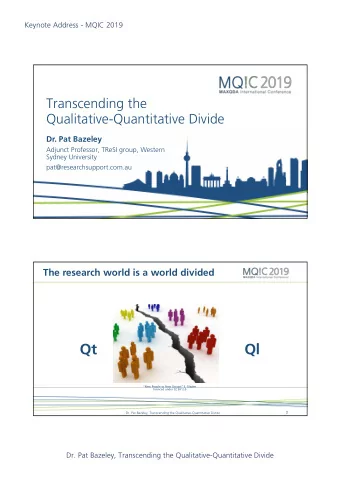
6/7/2018 Cell Free Fetal DNA in Maternal Plasma: A b i t o f b a c k g r o u n d … . Characteristics • O RI G I N P R I M A R I LY cffDNA represents ~10-15% of total DNA in maternal plasma 1 P L A C E N TA • R ES U LT S F RO M A P O P TO S I S Reliably detected after 7 wks gestation 2 • M A D E UP O F S HO RT S EG M E N T S O F F E TA L D N A Higher concentrations late in gestation ( < 2 0 0 BA S E PA I RS ) • C I RC U L AT E I N M AT E R N A L Short half life (16 min), undetectable by 2 hrs postpartum 3 P L A S M A cf DNA: The Future cfDNA: Common Clinical Applications Whole genome Aneuploidy : detect abnormal ratio of a particular testing chromosome Single gene Sex determination disorders Isoimmunization: noninvasively determine fetal Rh type Microdeletions 2
6/7/2018 Understanding the methods… D i f f e r i n g t e c h n i q u e s u s e d b y d i f f e r e n t l a b s Massively parallel shotgun sequencing (MPSS) Comprehensive Easy to add additional analyses Targeted sequencing Less expensive Single nucleotide polymorphisms (SNP) analysis Can distinguish maternal from fetal DNA Can identify triploidy, vanishing twin The less fetal DNA, the harder to tell normal from F r a c t i o n o f c f D N A t h a t i s fe t a l abnormal Prenatal Diagnosis 2012; 32(13) p 1233-41 3
6/7/2018 Cell free DNA screening: Biologic Challenges Cell free DNA screening: Biologic Challenges False Positives Unrecognized or “vanishing”twin False negatives Placental Mosaicism Low level of fetal DNA Low level maternal mosaicism, esp. sex chromosomes Placental mosaicism Maternal genetic variation (copy number variants) Maternal genetic variation (copy number Maternal Malignancy variants) Example of report and question Cell free DNA screening: Biologic Challenges Failed Results Increased BMI Low level of fetal DNA Fetal Aneuploidy 4
6/7/2018 P e r f o r m a n c e o f c f d n a f o r o t h e r a n e u p l o i d i e s What is the next step? A. No further testing needed, referral to GC to discuss diagnosis 55% B. Repeat cell free DNA 26% C. Recommend invasive testing 19% A g . N n . . D t i r s , e e d e e t r e d f e v l l i e e s n c a v g t n The false positives add up…. n a e i t i d p s e n e e t R m e r m h t o r c u e f R o N R a t e s o f a n o m a l i e s b y m a t e r n a l a g e Microdeletions are More Common Than Down Syndrome for Women Under 40 Adapted from: Snijders, et al. Ultrasound Obstet Gynecol 1999;13:167–170 5
6/7/2018 S h o u l d a l l w o m e n b e o f f e r e d Microdeletions are rare s c r e e n i n g f o r m i c r o d e l e t i o n s ? Expanded panels Trisomies 9, 16 and 22 Rarely seen in viable pregnancies except as mosaics Microdeletions • Microdeletions can be detected by cfDNA, but… 22q, 1q36, 5p-, 4p-, 15q11-13, 8q-, 11q- • Difficult to validate • Much of the data on in vitro samples Whole genome • Clinical testing includes small number of syndromes • 22q, 1q36, 5p-, 4p-, 15q11-13 (Prader-Willi/Angelman) 6
6/7/2018 Prevalence of many microdeletion syndromes is unknown Many such clinical syndromes are caused by different molecular mechanisms 95 cases were identified as Positive Only deletions detected 61 positives with follow up dx testing Smaller deletions more difficult to detect 22q syndrome (~1/4000) 11 true positives 50 false positives 85% have 3Mb deletion, 15% smaller “97% detection” refers to only 3Mb deletion Ultrasound Obstet Gynecol, 2016 cfDNA for Microdeletions Noninvasive Microarray Sequenced 565 samples: Prevalence of 5 microdeletion syndromes: ~1/2500 31 with CNV and 534 normal Prevalence of CNV by microarray: 1/60 • Detected 83% with CNV >6Mb but only 20% (2/10) that were <6Mb Detection rate of cfDNA for all pathogenic CNV: 4.2% • 2/534 false positives • More sequencing = higher sensitivity 7
6/7/2018 The false positives add up… Screening for these microdeletions has not been validated in clinical studies. Routine cell-free DNA screening for microdeletion syndromes should not be performed. T h e F u t u r e : N o n i n v a s i v e W h o l e G e n o m e S e q u e n c i n g • Coding and non coding portions • Single nucleotide variants • Deletions and Duplications • Copy number variants 8
6/7/2018 I s m o r e a l w a y s b e t t e r ? • OBTAIN INFORMATION ABOUT THE ENTIRE FETAL GENOME Ehrich et al. (2017) reports on the clinical experience of one lab’s experience with the • RAISES BOTH PRACTICAL AND first 10,000 cases ETHICAL ISSUES reports on copy number variations >7 Mb • MAY GIVE INFORMATION 25% of samples were sent due to an ultrasound abnormality REGARDING RISK FOR ADULT ONSET CONDITIONS THAT Screen-positive test results were reported in 554 cases, leading to a screen-positive rate ARE NOT RELEVANT of approximately 5.4% (compared with 2.3% in traditional cfDNA screening) However, pregnancy outcomes not available so no data on false positive or false negatives Non-Invasive Single Gene Tests C e l l f r e e D N A t e s t i n g f o r s i n g l e g e n e d i s o r d e r s Maternal and fetal cell free DNA cannot be easily distinguished Current clinically available for limited conditions Can identify de novo or paternal gene mutation circulating in maternal blood Achondroplasia An affected fetus will have an overrepresentation of the mutant allele in Thanatophoric dysplasia maternal plasma DNA Apert syndrome Ideal for autosomal dominant paternally inherited conditions Cystic fibrosis Useful if testing for an autosomal recessive condition and parents have different mutations 9
6/7/2018 Back to our case… Our patient underwent cell free DNA testing with micro deletions Her results were normal so she declined any further testing Level II ultrasound was notable for unilateral cleft lip and palate and abnormal profile Amniocentesis confirmed deletion of 8.9 MB deletion on 4p consistent with Wolf-Hirshorn Current guidelines ACOG/SMFM guidelines Conventional screening is most appropriate first line screen for most patients Ethically any patient may choose cfDNA screening, but should be counseled regarding limitations and benefits Diagnostic testing is required to confirm abnormal results before irreversible decisions Not recommended in twin pregnancies Special thanks to Mary Norton, MD Microdeletion/expanded panels for cell free DNA are not recommended 10
6/7/2018 11
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries