New Perspectives on the Pathogenesis of OSA - Anatomic Perspective - PDF document
New Perspectives on the Pathogenesis of OSA - Anatomic Perspective Richard J. Schwab, M.D. Professor of Medicine Interim Chief, Division of Sleep Medicine Medical Director, Penn Sleep Centers University of Pennsylvania Perelman School of
New Perspectives on the Pathogenesis of OSA - Anatomic Perspective Richard J. Schwab, M.D. Professor of Medicine Interim Chief, Division of Sleep Medicine Medical Director, Penn Sleep Centers University of Pennsylvania Perelman School of Medicine New Perspectives on the Pathogenesis of OSA: Anatomic Perspective - Disclosures • NIH grants - PPG (phenotyping and OSA) • ResMed Grant/Registry to study OSA/CSA and CPAP in hospitalized patients • Jazz clinical trial (JZP-110) for daytime sleepiness in OSA • Inspire CT study to examine upper airway anatomy with hypoglossal nerve stimulation 1
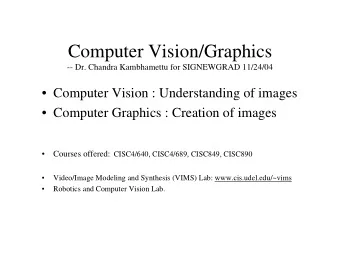
New Insights into the Pathogenesis of Sleep Apnea: Anatomic Perspective • Physical examination/anatomic risk factors for OSA • Anatomic pathogenesis of OSA – Increased size of upper airway soft tissues – Importance of tongue fat – Dynamic upper airway imaging during respiration Modified Mallampati Classification Class 1 Class 2 Class 3 Class 4 • Tsai et al, AJRCCM 167,1427-1432, 2003 • Mallampati et al. (1985). A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaest Soc J, 32(4), 429-34, 1985 2
Modified Mallampati Classification What is this patient’s Modified Mallampati score? Anatomic Risk Factors for Sleep Apnea • Obesity and its effects on the upper airway tissues • Increased neck circumference • Nasal airway restriction: septal deviation, allergic rhinitis, nasal polyps • Macroglossia/tongue ridging • Adeno-tonsillar hypertrophy (palatine/lingual tonsils) • Lateral peritonsillar narrowing • Enlargement/elongation of the soft palate • Recessed mandible (retrognathia)/maxilla • Narrowed hard palate - overbite/overjet • A combination of soft tissue and/or craniofacial risk factors is likely most important 3
Morphometric Measurements (Schellenberg AJRCCM 162;740-748, 2000) • Macroglossia: tongue being above level of mandibular occlusal plane • Uvula enlargement: > 1.5 cm in length or > 1.0 cm in width • Enlargement of lateral walls: > 25% impingement pharyngeal space by peritonsillar tissues • Tonsillar enlargement: > 50% lateral impingement of posterior pharyngeal airspace Normal Upper Airway (Schellenberg et al, AJRCCM 162;740-748, 2000) 4
Physical Examination and Sleep Apnea (Schellenberg et al, AJRCCM 162;740-748, 2000) Physical Examination and Sleep Apnea (Schellenberg et al, AJRCCM 162;740-748, 2000) 5
Normal Upper Airway (Schellenberg et al, AJRCCM 162;740-748, 2000) Lateral Pharyngeal Grading System • Class I = palatopharyngeal arch intersects at the edge of the tongue • Class II = palatopharyngeal arch intersects at 25% or more of the tongue diameter • Class III = palatopharyngeal arch intersects at 50% or more of the tongue diameter • Class IV = palatopharyngeal arch intersects at 75% or more of the tongue diameter Tsai, et al. A Decision Rule for Diagnostic Testing in Obstructive Sleep Apnea. American Journal of Respiratory and Critical Care Medicine, Vol. 167, No. 10 (2003), pp. 1427-1432 6
Physical Examination and Sleep Apnea (Schellenberg et al, AJRCCM 162;740-748, 2000) Narrowed Hard Palate and Sleep Apnea 7
Physical Examination and Sleep Apnea (Schellenberg et al, AJRCCM 162;740-748, 2000) Physical Examination and Sleep Apnea (Schellenberg AJRCCM 162;740-748, 2000) Adjusted Odds Ratio (OR) for Sleep Apnea Physical Finding OR 95% CI • Lateral Narrowing 2.6* 1.7 - 4.1 • Tonsillar hypertrophy 2.1* 1.1 - 4.2 • Macroglossia 2.0 1.1 - 3.6 • Enlarged soft palate 1.9 1.2 - 2.9 • Retrognathia 1.3 0.8 - 2.1 *Maintained significance after adjusting for BMI/neck size 8
Digital Morphometrics: A New Paradigm to Assess Upper Airway Anatomical Risk Factors for Obstructive Sleep Apnea ) Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi:10.1016/j.chest.2017.05.005 Quantify Anatomic Risk Factors for OSA with Digital Morphometrics/Laser Ruler Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi:10.1016/j.chest.2017.05.005 9
Upper Airway Soft Tissue and Craniofacial Measurements Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi:10.1016/j.chest.2017.05.005 Intraoral Photographs with Indicated Measures Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi:10.1016/j.chest.2017.05.005 10
Craniofacial Photograph with Laser Ruler The mandibular length is measured from the marked mandibular angle to the most prominent point on the chin Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi:10.1016/j.chest.2017.05.005 Examples of the Four Classes of Modified Mallampati • Class I indicates full visibility of the uvula and tonsillar fossa • Class II indicates visibility of upper portion of the uvula and partial visibility of the upper airway • Class III indicates visibility of the hard palate and base of the uvula • Class IV indicates visibility of the hard palate and no visibility of the soft palate Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi:10.1016/j.chest.2017.05.005 11
Digital Morphometrics: A New Paradigm to Assess Upper Airway Anatomical Risk Factors for Obstructive Sleep Apnea - Demographics All Patients Controls (AHI<10) Apneics (AHI≥10) Measure p N Estimate N Estimate N Estimate Age 844 47.4 ± 13.7 311 42.6 ± 13.9 533 50.2 ± 12.8 <0.0001 BMI 844 36.1 ± 9.9 311 32.1 ± 8.5 533 38.5 ± 9.9 <0.0001 Gender 0.027 Male 403 47.75% 133 42.77% 270 50.66% 441 52.25% 178 57.23% 263 49.34% Female Race 0.028 Caucasian 393 47.12% 155 50.49% 238 45.16% African 346 41.49% 110 35.83% 236 44.78% Other 95 11.39% 42 13.68% 53 10.06% AHI 844 26.3 ± 28.9 311 4.15 ± 2.83 533 39.2 ± 29.4 <0.0001 ln(AHI+1) 844 2.72 ± 1.18 311 1.45 ± 0.66 533 3.46 ± 0.67 <0.0001 Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi:10.1016/j.chest.2017.05.005 Digital Morphometrics: A New Paradigm to Assess Upper Airway Anatomical Risk Factors for Obstructive Sleep Apnea - Results All Patients Controls (AHI<10) Apneics (AHI≥10) Measure p N Estimate N Estimate N Estimate Modified Mallampati 0.017 Class I 35 4.59% 20 7.30% 15 3.07% Class II 79 10.35% 34 12.41% 45 9.20% Class III 126 16.51% 46 16.79% 80 16.36% Class IV 523 68.55% 174 63.50% 349 71.37% Airway Not Visible 649 85.06% 220 80.29% 431 87.73% 0.006 6.23 ± Mouth Width 792 6.17 ± 0.86 301 6.07 ± 0.86 491 0.012 0.85 5.16 ± Mouth Height 764 5.14 ± 1.04 291 5.09 ± 1.08 473 0.382 1.01 Mouth Area 771 24.0 ± 7.0 295 23.2 ± 7.4 476 24.4 ± 6.6 0.026 5.20 ± Tongue Width 726 5.12 ± 0.56 283 5.00 ± 0.52 443 <0.0001 0.57 Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi:10.1016/j.chest.2017.05.005 12
Digital Morphometrics: A New Paradigm to Assess Upper Airway Anatomical Risk Factors for Obstructive Sleep Apnea - Results All Patients Controls (AHI<10) Apneics (AHI≥10) Measure p N Estimate N Estimate N Estimate Mouth Width 709 6.01 ± 0.77 275 5.93 ± 0.81 434 6.07 ± 0.75 0.023 Tongue Width 782 5.23 ± 0.72 299 5.10 ± 0.71 483 5.30 ± 0.72 <0.001 Tongue Length 725 5.82 ± 1.23 270 5.85 ± 1.20 455 5.81 ± 1.26 0.680 Tongue Area 606 5.55 ± 1.94 236 5.39 ± 1.97 370 5.66 ± 1.91 0.099 Tongue Thickness 611 1.47 ± 0.30 239 1.41 ± 0.31 372 1.51 ± 0.28 <0.0001 Tongue Curvature 599 5.32 ± 1.24 235 5.35 ± 1.33 364 5.30 ± 1.17 0.642 Airway Width 146 2.18 ± 0.65 88 2.19 ± 0.61 58 2.15 ± 0.72 0.734 Uvula Length (Airway) 165 0.58 ± 0.27 91 0.56 ± 0.25 74 0.60 ± 0.30 0.302 Uvula Width (Airway) 351 0.89 ± 0.20 163 0.86 ± 0.18 188 0.91 ± 0.21 0.028 Uvula Area (Airway) 163 0.39 ± 0.22 89 0.35 ± 0.18 74 0.42 ± 0.24 0.046 Mandibular Length 731 7.38 ± 1.02 282 7.21 ± 0.94 449 7.48 ± 1.05 <0.001 Mandibular Width 652 9.99 ± 1.03 244 9.77 ± 0.98 408 10.11 ± 1.04 <0.0001 Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest, 152, 2017 Associations Between Photography Measurements and OSA and AHI - Conclusions • Apneics had higher scores on all measures of Mallampati, less airway visibility, larger mouth width and area, and larger tongue width and thickness • Also had more severe pharyngeal narrowing within the subpopulation where this measure was quantifiable • Measurements of intraoral crowdedness showed the strongest associations in OSA and AHI status • Apneics tended to have more crowded or less visible airways than controls Schwab, R. et al., (2017). Digital Morphometrics: A New Upper Airway Phenotyping Paradigm in OSA. Chest., 152(2). doi:10.1016/j.chest.2017.05.005 13
Recommend












More recommend
Explore More Topics
Stay informed with curated content and fresh updates.