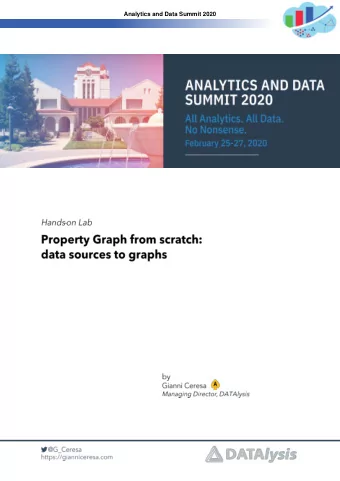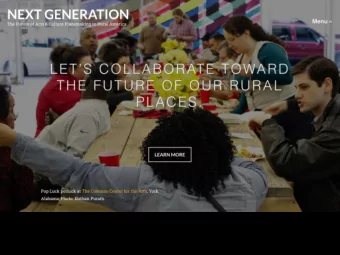
MidSouth’s Current Year 4 Aim 2 Aim 1 Improve Health Enrollment Performance on TCPi Aims Outcomes Improve health outcomes of Medicare, Medicaid Support clinicians in their practice and other patients. MidSouth PTN achieved 267% transformation work. MidSouth PTN of our target already. successfully enrolled 109% of our target of 4050 clinicians. Aim 3 Aim 4 Reduce Generate Savings Unnecessary Hospitalizations Reduce unnecessary hospitalizations for Generate savings to the federal government and Aim 1 commercial payers. MidSouth PTN generated patients. MidSouth PTN has already avoided 100 over 20,000 unnecessary hospitalizations, more than $174 million in cost savings, representing 121% of our target. meeting 87% of our target. 80 Aim 7 Aim 2 Aim 6 Aim 5 60 Transition Practices Reduce 40 To APMs unnecessary Tests 20 Sustain efficient healthcare delivery by reducing Transition 75% of practices into APMs. MidSouth unnecessary tests and procedures. MidSouth PTN PTN has already accomplished 38% of that 0 far exceeded our target, reducing over 17,000 target, transitioning 31 practices into APMs. unnecessary tests and procedures, representing Aim 6 Aim 3 1379% of our target. Aim 7 Transform Practice Beyond Phase 3 Aim 5 Aim 4 Build the evidence base of practice transformation so that effective solutions can be scaled. MidSouth PTN has transformed 64% of our practices beyond phase 3.
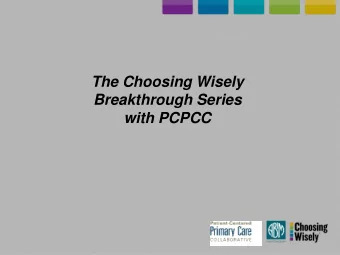
VHAN’s Current Year 4 Aim 1 Enrollment Performance on TCPi Support clinicians in their practice transformation work. To date, VHAN has enrolled 65% of our Aims current clinicians. Aim 6 Aim 1 Transition Practices 100 To APMs 80 Transition 75% of practices into APMs. VHAN has Successfully transitioned 15 practices to APMs Aim 7 Aim 2 60 40 20 0 Aim 7 Aim 6 Aim 3 Transform Practice Beyond Phase 3 Build the evidence base of practice transformation so that effective solutions Aim 5 Aim 4 can be scaled. VHAN has transformed 30 practices beyond phase 3!
Supporting and What is VBCU? • Sustaining Our A curriculum to inform and prepare front line staff (QIAs), o providers, and executives for implementing value-based care (VBC) Practices’ Work What’s on the agenda? • • Value- based care landscape, “101” and history • Key concepts of pay for volume to pay for value • Available models in the payer space Value Based Care • Fiscal risks and payoffs • Connecting clinical outcomes to fiscal performance University • Practice change management • The horizon ahead for VBC When does VBCU start? • August 16, 2019 • How do I learn more? • Email us at: midsouthptn@vumc.org •
Supporting and Sustaining Our MidSouth Media/PR Team Practices’ Work Mission: An active legacy defining the future of healthcare. Vision: Telling the Story of Our Success Create a living, replicable body of Performance stories • knowledge for practices to leverage as they Social media • MidSouth has dedicated our final take their transformation journeys from fee- Videos • year to creating an active legacy of for-service to value-based care. “Best Practices” Podcast • our transformative, four year Summer Summits • partnership with CMS through TCPI.
REGIONAL KEYNOTE C.J .J. Stim imson, MD, JD Assistant Professor, Urologic Surgery (VUMC) Medical Director, Office of Episodes of Care, Population Health Senior Advisor to Chief Health System Officer (Vanderbilt Health) Senior Advisor to the Front Office for the Center for Medicare and Medicaid Innovation (CMMI)
The Future of Value-Based Care C.J. Stimson, MD, JD
Disclosures The views expressed in this presentation are my own, and do not necessarily reflect the positions of the Center for Medicare & Medicaid Services, the Vanderbilt Health Affiliated Network, or Vanderbilt University Medical Center.
Outline 1. Fake News: Value is Dead 2. Purchaser-Driven Value 3. Patient-Driven Value
Conclusions Value is here to stay. Purchasers and patients will drive the value transformation.
Fake News: Value is Dead
Fake News: Value is Dead
Fake News: Value is Dead Why?
Fake News: Value is Dead
Fake News: Value is Dead Why else?
Fake News: Value is Dead “[I] insist CMMI… “if [a model] needs to be mandatory cease all current and future planned opposed [sic] to mandatory voluntary to get initiatives within adequate data, then CMMI” so be it.” - Alex Azar - Tom Price, et al September 2016 January 2018
Fake News: Value is Dead The real story?
Fake News: Value is Dead Value is here to stay.
Purchaser-Driven Value
Purchaser-Driven Value Purchasers will continue to push providers to drive down spend while maintaining or improving quality.
Purchaser-Driven Value
Purchaser-Driven Value
Purchaser-Driven Value
Purchaser-Driven Value
Purchaser-Driven Value
Purchaser-Driven Value
Purchaser-Driven Value
Purchaser-Driven Value
Purchaser-Driven Value
Purchaser-Driven Value
Purchaser-Driven Value
Purchaser-Driven Value What does all of this mean?
Purchaser-Driven Value Purchasers will drive the value transformation.
Patient-Driven Value
Patient-Driven Value Empowering and engaging patients to drive value and disrupt market share.
Patient-Driven Value Empowering and engaging patients to driv rive valu lue and disrupt market share.
Patient-Driven Value Empowering and en engaging patients to drive value and dis isrupt mark rket share .
Patient-Driven Value – Empowering Empowering patients to driv rive value lue.
Patient-Driven Value – Empowering
Patient-Driven Value – Empowering
Patient-Driven Value – Empowering 61
Patient-Driven Value – Empowering
Patient-Driven Value – Empowering
Patient-Driven Value – Empowering
Patient-Driven Value – Empowering Confidential. Do Not Distribute.
Patient-Driven Value – Engaging Engaging patients to dis isru rupt mark rket sha hare.
Patient-Driven Value – Engaging
Patient-Driven Value – Engaging
Patient-Driven Value – Engaging Confidential. Do Not Distribute.
Patient-Driven Value – Engaging
Patient-Driven Value What does all of this mean?
Patient-Driven Value Patients will drive the value transformation.
Conclusions
Conclusions Value is here to stay. Purchasers and patients will drive the value transformation.
SHOWCASE of PRACTICES
The Grove Primary Care Cli linic Whole Pers erson Care Prim imary Ca Care Practice 12 Pro rovid iders Date te Jo Join ined TC TCPI: I: 05/01/2017 Specific TCPI AIMS Impacted Through This Work: 2: Improved health outcomes 3: Reduce unnecessary hospitalizations https://vimeo.com/338903929/b586e731e4 4: Generate savings
OBGYN Associa iates Hydration Campaign to Reduce Visits to L&D for Pregnant Patients OBGYN Specialty Practic ice 9 Pro rovi viders Date te Jo Join ined TC TCPI: I: 03/28/2016 Specific TCPI AIMS Impacted Through This Work: 2: Improved health outcomes 3: Reduce unnecessary hospitalizations 4: Generate savings
OBGYN Associa iates HYDRATION CAMPAIGN • An analysis of the L&D data for revealed that 75% the patients going to L&D, who did not deliver, were seen for conditions or complications related to dehydration. • Poster created and reviewed with patients, posted in the lobby and exam rooms • Clinical Staff trained on specific instructions/scripting around hydration for incoming patient phone calls • Decreased ED / L&D Visits by 4.3%
Womens Group of Franklin in Th The Rig ight Care re at t th the Rig ight Tim Time Specia ialt lty Ca Care re Pra ractic ice 10 Pro rovid iders Date te Jo Join ined TC TCPI: I: 04/06/2016 Specific TCPI AIMS Impacted Through This Work: 2: Improved health outcomes 3: Reduce unnecessary hospitalizations https://vimeo.com/339635905/da7ee38eb7 4: Generate savings
Main in Street Famil ily Medicin ine Opioid Rx Reduction Pri rimary Ca Care re Pra ractice 4 Provi viders Date te Jo Join ined TC TCPI: I: 03/17/2016 Specific TCPI AIMS Impacted Through This Work: 2: Improved health outcomes 5: Reduce unnecessary testing and procedures 7: Build the evidence base to scale solutions
Main in Street Famil ily Medicin ine Opioid Rx Reduction Initiative • Analyzed a years worth of prescribing patterns, by provider, to develop a baseline • Developed opioid prescribing protocol No opioid prescriptions for new patients No opioids prescribed on weekends No swapping out prescriptions between providers Opioid patients required to come in for a visit once a month Chronic pain patients required to sign pain management agreement or referred to pain management clinic Rx <120 Morphine Milligram Equivalent (MME) per patient, preferably < 90
Main in Street Famil ily Medicin ine Opioid Rx Reduction Initiative From November 2018 - February 2019, the practice saw a 65% decrease in the overall MME prescribed. Each of the individual providers also saw a decrease.
Upper Cumberland Famil ily Physicians Ded edicated Vis isits fo for r Dia iabetic Pati tients Pri rimary Ca Care re Pra ractice 6 Pro rovi viders Date te Jo Join ined TC TCPI: I: 02/08/2016 Specific TCPI AIMS Impacted Through This Work: 2: Improved health outcomes 3: Reduce unnecessary hospitalizations 4: Generate savings https://vimeo.com/338901890/3c1c436ce5 5: Reduce unnecessary testing and procedures
Dr. . Frances Berry-Brown Paja jama-time PDSA: Decreasing Aft fter-hours Paperwork and In Inefficiencies Pri rimary Ca Care re Pra ractice 1 Pro rovi vider Jo Join ined TCP CPI: I: 04/0 /04/2016 Specific TCPI AIMS Impacted Through This Work: 1: Support physician practice transformation 3: Improve health outcomes 4: Generate savings
Dr. . Frances Berry-Brown Paja jama-time PDSA: Dec ecreasing Aft fter-hours Paperwork and In Inef effi ficiencies • EMR Training & Process Standardization ▪ Optimized reporting ▪ Messaging and team member assignments ▪ Referrals ▪ Check-out process ▪ Standardized templates (office notes, order sets, patient instructions) • Daily Huddles ▪ Review schedule for the day ▪ Clarify task assignments ▪ Close gaps ▪ High-priority messages • Staffing Role Definition
Cookevil ille le Coll llaborative TC TCPi Success Sto tory & Bes est Pra ractice Coll llabora rative Even ent Hig ighlights Specific TCPI AIMS Impacted Through This Work: 1: Support clinicians in their practice transformation work 2: Improved health outcomes 4: Generate savings 5: Reduce unnecessary testing and procedures https://vimeo.com/339613801/48a2ce9522
Terrace Pediatric Group Im Impacting Avoidable ER Utilization Pediatr tric Practic ice 4 Pro rovi viders Date te Jo Join ined TC TCPI: I: 02/18/2016 Specific TCPI AIMS Impacted Through This Work: 2: Improved Health Outcome 3: Reduce Unnecessary Hospitalizations 4: Generate Savings 5: Reduce Unnecessary Testing and Procedures
Terrace Pediatric Group Im Impacting Avoidable ER Utiliz tilization • Da Data analy lysis of of Q4 2016 reve revealed a baseline of of 14.8 .81% of of patie ients were ere repo reporting to o the he ER ER ▪ Incl ncluded TennCar are as as well ll as as Commercial al paye payer patie patients • Coll llected lis ist of of ED ED locations whe here patie ients were ere see seen • Det Determin ined if/how not notifi fications were ere bein eing sent sent by y hos hospit itals to o prac ractice offic office • Coll llected data and plan deve eveloped for or foll ollow-up prot rotocol • Init itial Foll Follow-up Pro rotocol was deve evelo loped and implemented ▪ ED ED patie patient t list list (dai daily ly), ), Nur Nurse follo low-up phon phone ca calls lls and and appo appoin intments s made ade as as appr appropriate te, MD noti notified for inpu input • Seco Second iteratio ion of of Fol Follo low-up Pro rotocol was deve eveloped and imple lemented ▪ Incl ncluded patie patient t edu ducati ation, im impr proved doc documentat tation re regar arding atte attempts ts to to co cont ntac act t patie patient, t, tigh tighter diagn diagnosis foll llow-up param parameters, sign sign-off f by by MD if if no no foll llow-up ne needed
Terrace Pediatric Group Im Impacting Avoidable ER Utiliz tilization 14.0% Target 14.1% • Da Data trend rended dow ownward from rom 14.8 .81% in Q4 2016 to o 8.3 .3% in Q1 2019. • We e did see see an upt uptic ick in Q4 and Q1 ea each year year, we e attribute this his to o co cold ld/fl flu se season
Gallatin Women’s Center Gallatin Women’s Center’s Transformation Jo Journey Specia ialt lty Ca Care re Pra ractic ice 5 Pro rovi viders Date te Jo Join ined TC TCPI: I: 04/18/2017 Specific TCPI AIMS Impacted Through This Work: 1: Support Transformation 3: Reduce unnecessary hospitalizations 4: Generate savings
Gallatin Women’s Center Tra Transfo formation Jo Journey • Continuous Data-Driven Quality Improvement • Sustainable Business Operations • Team-based relationships & Efficiency of operation • Person and Family-Centered Care Design QI Committee Daily Huddles August 2018 April 2019 Budget Community November 2018 Health Worker May 2019
BREAK TIM IME Ple lease return by 12:0 :00
LUNCH 12:0 :00 -12:4 :45
A Reflection on our TCPi Journey…
CMS KEYNOTE Robert Fle lemming, PhD Director of the Transforming Clinical Practice Initiative at The Centers for Medicare and Medicaid Services
CLOSIN ING REMARKS Cynthia ia Powell, l, MD Medical Director, Population Health
Our Goals Redesigning Care and Strengthening Communities The Our network includes hospitals, physician practices, clinics, and post-acute care facilities across Tennessee and surrounding states. Our mission Vanderbilt is to improve care across the Southeast by equipping providers to succeed in population health and sharing evidence-based best practices. Net etwork Highlig lights: Health • More than $25 million in costs avoided for health plans Affiliated • $12 million in shared savings to network clinicians • Consistent cost savings and quality performance for four years running Network Transforming Improving Health & Driving We are a collaborative alliance of providers committed to transforming Care Delivery Productivity Innovation healthcare. From flu shots to the most complex care, we are working together We have built a high-quality network of providers Network providers use data-driven approaches to We work with insurance companies, brokers, and to make healthcare more proactive, who are transforming the practice of medicine by engage patients and offer access to the care they employers to create value-based solutions for focusing on care quality and value. need, when and where they need it. managing workforce health and employee accessible, and affordable. benefits. MORE By creating innovative solutions and Quality partnerships with clinicians, care THAN employers, and insurance carriers, we for more 6,700 are improving the quality and value of than Millions 350,000 healthcare across the Southeast. in sharedsavings providers participating in delivered to health plan sponsors and patients across Tennessee our high-quality network and surrounding states network clinicians for 4 years running Managing the Total Cost of Care By transforming care delivery, improving health and productivity, and driving innovation, we’re effectively managing the total cost of care. As a result, our model delivers high value while reducing healthcare costs.
The Largest Network in the Region The Vanderbilt Health Affiliated Network is driving a new level of clinical innovation and teamwork to bring high-quality, accessible healthcare and services to communities in Tennessee and surrounding states. The network includes more than 6,700 clinicians, 68 hospitals, 13 health systems, and hundreds of physician practices and clinics working together to provide the best care, at the right time, and at the right cost. Hospitals 24 472 13 39 PrimaryCare 23 44 890 88 Providers QuickCare Clinics 16 338 21 30 Post-Acute CareFacilities WEST: Baptist Memorial Health Care • West TennesseeHealthcare MIDDLE TENNESSEE: Cookeville Regional Medical Center • Jennie Stuart Health • LifePoint Tennessee Hospitals • Maury Regional MedicalCenter NorthCrest Health • Saint Thomas Midtown • Saint Thomas Rutherford • Sumner Regional Medical Center • Vanderbilt University Medical Center • Williamson Medical Center EAST: Erlanger Health System • Mountain States Health Alliance • University of Tennessee MedicalCenter Contact us at vhan.com or call 1-877-969-3194.
Our Goals Ensure the Ens he ri right ca care Improve appropriateness Decrease unnecessary variation Creating Ens Ensure the he hig highest quali lity ca care Improve outcomes and experience Healthcare Reduce the Red he tota otal co cost of of car care Valu lue Pos osit itio ion VH VHAN as as the he prefe referred fin inancially ly su sustain inable le inte ntegrated he health sy system
Our Approach Care re Deliv elivery Models ls RN, Care Team-based care Coordinator High value care coor dination Community LPNs/ Transitions of care Health MAs Worker Inte Integrated Care Te Team A multidisciplinary approach to care Patient/ Family Social Work Provider Cont ntin inuous Qua ualit lity and nd Pro rocess ss Im Improvement Partner to redesign and improve care delivery Data collection, analysis, and reporting Standard care processes that can be measured Data Pharmacy Analyst Communit ity Eng Engagement Align community health strategies Integration of community resources
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries