
MENTAL HEALTH & DADS CONTRACTOR EHR PLANNING MEETING May 25, - PowerPoint PPT Presentation
MENTAL HEALTH & DADS CONTRACTOR EHR PLANNING MEETING May 25, 2011 AGENDA Welcome & Introductions Breakout Sessions MH & DADS Funding Methodology Funding Application Bring MH and DADS back together Next
MENTAL HEALTH & DADS CONTRACTOR EHR PLANNING MEETING May 25, 2011
AGENDA Welcome & Introductions Breakout Sessions MH & DADS Funding Methodology Funding Application Bring MH and DADS back together Next Steps Concurrent EHR Planning Sessions 2
DADS AND MENTAL HEALTH BREAKOUT SESSINS 3
FUNDING & FUNDING PROCESS County & Contractor Methodology Committee Purpose: Develop and implement a methodology and criteria to be used in allocating available funds to Mental Health Short Doyle contract agencies for their transition to an electronic health record (EHR) system. 4
COMMITTEE PRINCIPLES Funding should be reviewed in relation to meeting minimum requirements for all agencies. All current Short Doyle Mental Health Contractors will be considered for some MHSA Technological Needs funding based on need. 5
COMMITTEE MEMBERS Bruce Copley Deputy Director MHD / County Sponsor Liaison Sheila Yuter County MHD / Committee Co‐Chair Erin O’Brien AMCHA / Committee Co‐Chair Jorge Wong AACI / AMHCA Member Rachel Clausen EMQ Families First / AMHCA Member Michael Hutchinson County DADS / QI Clinical Standards Terry Boyle Unity Care / Non AMCHA “At large” Member Bruce Fielding Children’s Health Council / “At large” Member Alyce Cobb County MHD Contract Monitor Lauren Gavin County MHD Contract Monitor Sue Clements County EHR Project Manager Tony Perez County Procurement Department Martha Paine County General Fund Finance Director Christine Trong Pathway Society / DADS Gina Trepagnier Hope Services / Small Agency Representative 6
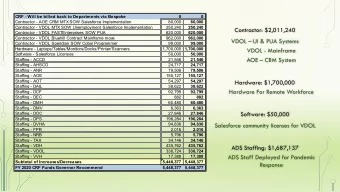
FUNDING METHODOLGY SCCo will have up to $4M to award to contractors Amounts are “not to exceed” and will be considered planning estimates, not fixed amounts Planning estimates will be based on ‐‐ Meeting EHR minimum requirements Agency’s need specifically related to meeting EHR minimum requirements by December 31, 2013 7
FUNDING METHODOLOGY General approach Smaller agencies may be awarded more than larger ones, but no award will be more than 20% of an agency’s annual SCCo Mental Health budget A blended formula was used to determine planning estimates consisting of ‐‐ an even distribution of one half of the available funds, plus a percent of the remaining half, the percent being inversely proportional to the size of the agency Again, no agency’s planning estimate may exceed 20% of total agency MH budget 8
APPLICATION PROCESS Applications will be accepted between June 1 and December 30, 2011 The application for funding contains three parts: General information Statement of readiness Budget 9
READINESS New or existing system? ASP (contract for external service) or Self Host (own and maintain yourself)? Complete minimum requirements checklist Provide implementation plan and timeline Provide signed (or to be signed) contract % of your budget that is used for SCCo MH
REVIEW AND AWARD Applications will be reviewed by MH and IT staff Individual meetings to discuss proposal Expect up to 8 weeks to process and develop contract
MINIMUM REQUIREMENTS The minimum requirements for an EHR and electronic data exchange that must be met to receive County funds. County will further define the data that will be necessary to meet these requirements; including data format and method for which the County will receive the secure HIPAA compliant files 13
MINIMUM REQUIREMENTS For each requirement, indicate if it is: Existing: Already installed and/or in use In Progress: Is in the process of being installed and/or used Planned: Is being planned for in the future. Implementation Date: For requirements that are in progress or planned , please indicate the estimated date for completion. 14
MINIMUM REQUIREMENTS The minimum requirements for an EHR and electronic data exchange that must be met to receive County funds. County will further define the data that will be necessary to meet these requirements; including data format and method for which the County will receive the secure HIPAA compliant files 15
MINIMUM REQUIREMENTS For each requirement, indicate if it is: Existing: Already installed and/or in use In Progress: Is in the process of being installed and/or used Planned: Is being planned for in the future. Implementation Date: For requirements that are in progress or planned , please indicate the estimated date for completion. 16
MINIMUM REQUIREMENTS # Requirement 1 Certified EHR 2 Security & Privacy 3 Client ID 4 Claim Information 5 Reporting Data (CSI/CALOMS/Other) 6 Additional Demographics 7 Problem List 8 Outcome Measures (e.g. MORS) 9 Transition Care / Referrals 17
MINIMUM REQUIREMENTS # Requirements 10 Electronic Audit Capability 11 Progress Notes 12 Treatment Plans 13 e‐Signature 14 CPOE (Computer Physician Order Entry) 15 e‐Prescribing 16 Maintain Active Medication List 17 Vital Signs 18 Maintain Active Allergy List 19 Consents 18
19
EHR PLANNING SESSION #1 Information for those that are in the early stages of planning. This session will cover Where do you begin? Technical Considerations Vendor Demo and Evaluations Vendor Comparison Costs 20
EHR PLANNING SESSION #2 Information for those that are in the early stages of planning. This session will cover: Culture Change Common Risks Project Sponsorship Project and Work Teams Training Productivity Vendor Performance And more… 21
EHR Planning Session #1 Early Planning 22
EHR Planning Session #1 Information for those that are in the early stages of planning. This session will cover Where do you begin? Technical Considerations Vendor Demo and Evaluations Vendor Comparison Costs 23
24
Where do you begin? What’s Needed to Get Started? Start talking about the EHR as a positive change Prepare staff for changes Pull Your Team Together Pick a driver (Agree on the driver) Include varying disciplines Set up ongoing meetings Create realistic timelines 25
Readiness Assessment Go through the assessment as a team Take note where the team does not agree Recognize areas of need and follow up Refer back regularly Track change 26
Workflow and Needs Track how a client moves through the system Receiving Referral Treatment Billing/Payment Discharge You want to recognize where the system fails and succeeds This will help you identify where an EHR may provide improved efficiency, accuracy and better client care You want a tool that works for you. You don’t want to work for the tool 27
28
Internal Capabilities What shape is your IT Department in? Do you have an IT Department? Who will own the EHR system internally? Program or Support? Do you currently have some sort of an EHR system? What is the reputation of the existing system? 29
Technology Assessment Do you feel the need for speed? Cable, T1, Ethernet ready? Who is in charge? Do you have someone identified to be primary interface? Spread the love Test and Validate with several sets of eyes 30
Technology Assessment Does Staff know what a computer is? Training capabilities Does Staff have the time? Redesign workflow Implement the system Validate results Repeat 31
Budget Considerations Compreh ensive Cost Estimate Cost of System or Licensing Fees 3 rd Party Products and Services Annual Support Implementation Services Cost Hardware Internal Staff Project Manager Systems Analyst Database Administrator / Trainer 32
Budget Considerations Comprehensive Cost Estimate (continued) External Consultants Lost Productivity Before, During and After Initial Implementation Custom Programming Fees Scalability Adding users in the future Security 33
Buy v. Rent Buy Internally Hosted on Your Server Higher Upfront Costs Nominal Recurring Costs Rent ASP (Application Service Provider) SaS (Software as a Service) Remotely Hosted via Internet Low Upfront Costs Continuous Recurring Costs 34
Buy v. Rent Buy Not Internet Reliant Quicker Response / Access Time Capital Expenditure v. Operating Costs Data control Rent Access from any place with Internet access Nominal worries about backups, updates, etc. Upgrades usually built into monthly charge Less maintenance / IT dependant 35
36
Recommend










More recommend
Explore More Topics
Stay informed with curated content and fresh updates.