Management of Management of Hypertension Hypertension M Misra MD MRCP (UK) M Misra MD MRCP (UK) Division of Nephrology Division of Nephrology University of Missouri School of University of Missouri School of Medicine Medicine
Disturbing Trends in Disturbing Trends in Hypertension Hypertension � HTN awareness, treatment and control rates HTN awareness, treatment and control rates � are decreasing are decreasing � Age adjusted mortality rates for stroke and Age adjusted mortality rates for stroke and � CHD appear to be either rising or leveling of CHD appear to be either rising or leveling of � The incidence of ESRD and the prevalence of The incidence of ESRD and the prevalence of � CHF is increasing CHF is increasing � HTN related complications are a public health HTN related complications are a public health � concern concern � Treatment of HTN is a worldwide failure! Treatment of HTN is a worldwide failure! �
Mechanics of Mechanics of Hypertension Hypertension � Primary salt factor: Primary salt factor: � suppressed renin renin suppressed good response to a diuretic good response to a diuretic � Primary Primary Renin Renin Angiotensin Angiotensin factor: factor: � elevated renin renin elevated good response to antirenin antirenin- -angiotensin angiotensin good response to type medication type medication
Blood Pressure and Blood Pressure and Cardiovascular Risk Cardiovascular Risk Relationship between BP and Relationship between BP and Cardiovascular risk Cardiovascular risk Strong Strong Continuous Continuous Graded Graded Consistent Consistent Independent Independent Predictive Predictive Etiologically significant Etiologically significant
Why treat? Why treat? � Hypertension is deleterious to the vascular Hypertension is deleterious to the vascular � health health � Evidence Evidence from natural experiments in from natural experiments in � humans: Unilateral RVD Unilateral RVD humans: Coarctation of aorta Coarctation of aorta Pulmonary hypertension Pulmonary hypertension � Evidence Evidence from animal experiments from animal experiments � � Evidence Evidence from Clinical trials from Clinical trials �
Variables in Treatment Variables in Treatment and/ or Response and/ or Response � Race / ethnicity Race / ethnicity � � Age Age � � Sex Sex � � Co Co- -morbidity morbidity � � Co Co- -treatment treatment �
Management Objectives Management Objectives Cause � Identify Identify Cause � Cardiovascular Risk � Identify other Identify other Cardiovascular Risk � Factors Factors Target Organ Damage � Assess Assess Target Organ Damage � Cardiovascular Disease. � Assess Assess Cardiovascular Disease. �
Classification of Hypertension in adults (>18years)
Identifiable causes of Hypertension Identifiable causes of Hypertension � Sleep Apnea Sleep Apnea � � Drug induced/related Drug induced/related � � Chronic Kidney Disease Chronic Kidney Disease � � Primary Primary aldosteronism aldosteronism � � Renovascular Renovascular disease disease � � Cushings Cushings/chronic steroid therapy /chronic steroid therapy � � Pheochromocytoma Pheochromocytoma � � Coarctation Coarctation of aorta of aorta � � Thyroid or Thyroid or hyperparathyroid hyperparathyroid disease disease �
Lifestyle modifications for Hypertension
Renal Diseases in Hypertension Renal Diseases in Hypertension Core Concepts of Treatment Core Concepts of Treatment � Hypertension Hypertension is an independent variable that is an independent variable that � predicts long- -term decline in renal function term decline in renal function predicts long � Proteinuria Proteinuria is also an independent variable that is also an independent variable that � predicts long- -term decline in renal function term decline in renal function predicts long � Reduction of blood pressure reduces both Reduction of blood pressure reduces both � cardiovascular and renal risk cardiovascular and renal risk � Reduction of Reduction of proteinuria proteinuria may reduce both may reduce both � cardiovascular and renal risk cardiovascular and renal risk � Relative renal Relative renal hypoperfusion hypoperfusion during initial stages of during initial stages of � therapy for hypertension is associated with a therapy for hypertension is associated with a transient limited rise in serum creatinine and is not transient limited rise in serum creatinine and is not a reason to stop therapy a reason to stop therapy
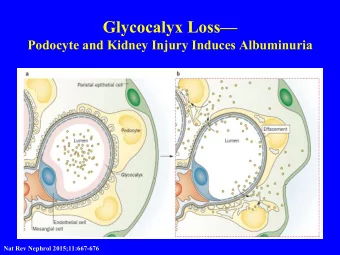
The Dual Significance of Proteinuria The Dual Significance of Proteinuria � Proteinuria ( Proteinuria (albuminuria albuminuria) results from injury ) results from injury � to glomerular circulation to glomerular circulation � Increased proteinuria ( Increased proteinuria (albuminuria albuminuria) is ) is � associated with progressive kidney disease associated with progressive kidney disease � In diabetes and hypertension, proteinuria In diabetes and hypertension, proteinuria � (albuminuria albuminuria) is also an indicator of injury in ) is also an indicator of injury in ( the systemic circulation the systemic circulation � Proteinuria ( Proteinuria (albuminuria albuminuria) is associated with ) is associated with � increased cardiovascular risk increased cardiovascular risk
Definitions of Microalbuminuria Microalbuminuria Definitions of and Macroalbuminuria Macroalbuminuria and Micro- - Macro- - Micro Macro Parameter Normal Parameter Normal albuminuria albuminuria albuminuria albuminuria Urine AER Urine AER < 20 20 - - 200 200 > 200 < 20 20 > 200 ( μ μ g/ min) g/ min) ( Urine AER Urine AER < 30 30 - - 300 300 > 300 < 30 30 > 300 (mg/ 24h) (mg/ 24h) Urine Urine albumin/ albumin/ < 30 30 - - 300 300 > 300 < 30 30 > 300 # ratio Cr # ratio Cr (mg/ gm) (mg/ gm) AER= Album in excretion rate CR # = creatinine
Goal BP Recommendations for Goal BP Recommendations for Patients with DM or Renal Disease Patients with DM or Renal Disease Systolic Diastolic Year Systolic Diastolic Organization Organization Year BP BP BP BP < 130 < 80 American Diabetes Association 2001 < 130 < 80 American Diabetes Association 2001 < 130 < 130 < 80 < 80 National Kidney Foundation National Kidney Foundation 2000 2000 < 130 < 80 Canadian Hypertension Society 1999 < 130 < 80 Canadian Hypertension Society 1999 < 140 < 80 British Hypertension Society 1999 < 140 < 80 British Hypertension Society 1999 WHO & International WHO & International < 130 < 85 1999 < 130 < 85 1999 Society of Hypertension Society of Hypertension Joint National Committee Joint National Committee < 130 < 85 1997 < 130 < 85 1997 (JNC VI) (JNC VI)
Drug Therapy Drug Therapy � Avoid overdosing Avoid overdosing � � Avoid Quick Fix (cerebral and Avoid Quick Fix (cerebral and � coronary hypoperfusion may result) coronary hypoperfusion may result) � Aim for 24 hour coverage Aim for 24 hour coverage �
Drug Therapy Drug Therapy � Minimize Side Effects Minimize Side Effects � � Establish goal Establish goal � � Educate Educate � � Maintain contact Maintain contact � � Keep care inexpensive Keep care inexpensive � � Favor longer acting medications Favor longer acting medications � � Be willing to change Be willing to change �
Anti- -Hypertensive Drugs: Hypertensive Drugs: Anti Sites of Action Sites of Action Total Blood Cardiac = X Peripheral Pressure Output Resistance β - ACE I nhibitors Blockers AT 1 Blockers a-Blockers a 2 -Agonists CCBs * CCBs Diuretics Diuretics Sym patholytics Vasodilators * = non-dihydropyridine CCBs
Average Number of Anti- -Hypertensive Hypertensive Average Number of Anti Agents Used to Achieve Target BP Agents Used to Achieve Target BP MDRD ABCD HOT UKPDS MDRD ABCD HOT UKPDS < 92 < 75 < 80 < 85 < 92 < 75 < 80 < 85 mmHg mmHg mmHg mmHg mmHg mmHg mmHg mmHg Goal BP Goal BP MAP* MAP* DBP DBP DBP DBP DBP DBP Achieved BP 93 ~ 75 81 82 Achieved BP 93 ~ 75 81 82 Avg # of # of Avg drugs per 3.6 2.7 3.3 2.8 drugs per 3.6 2.7 3.3 2.8 patient patient * The goal m ean arterial pressure ( MAP) of < 9 2 m m Hg specified in the MDRD trial corresponds to a systolic/ diastolic blood pressure of approxim ately 1 2 5 / 7 5 m m Hg.
Diuretics Diuretics � Action Action : Decrease plasma volume and : Decrease plasma volume and � TPR. TPR. � Effect Effect : D : Decrease overall CV mortality. ecrease overall CV mortality. � � Side effects Side effects : Mainly metabolic : Mainly metabolic � � Start with a thiazide diuretic (low dose Start with a thiazide diuretic (low dose � combinations) combinations) � Loop diuretics required if serum Cr > 2.5 Loop diuretics required if serum Cr > 2.5 � mg/dl mg/dl
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries