
SLIDE 1
2/13/2018 1
Management Issues in Hypoglossal Stimulation for OSA
Kingman P Strohl M.D.
Professor of Medicine, Physiology & Biophysicis, and Oncology Center for sleep Disorders Reseach Case Western Reserve University, Cleveland OH, USA
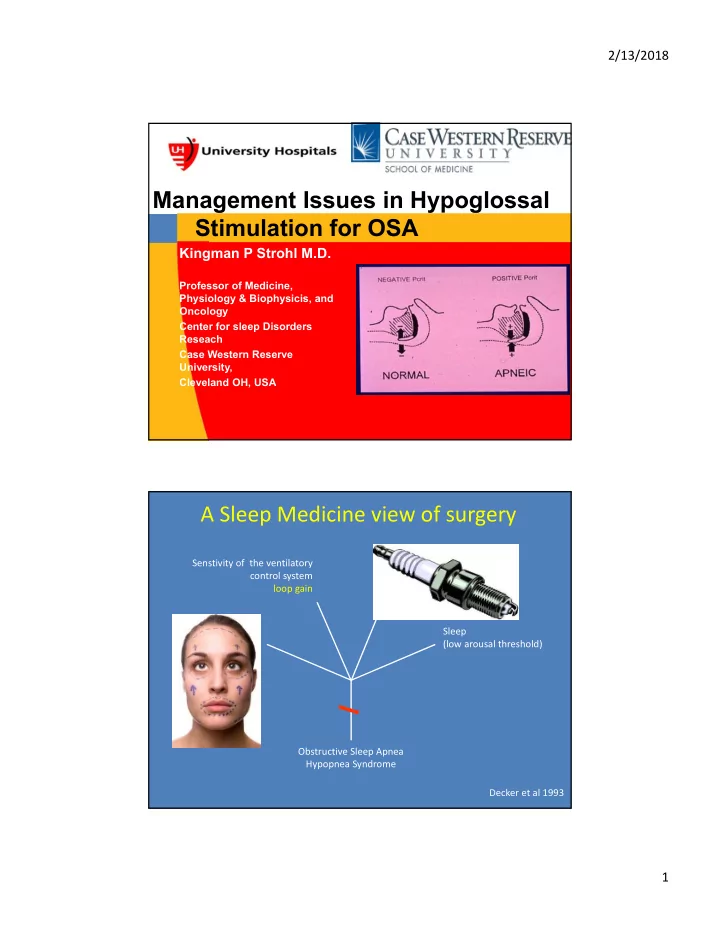
A Sleep Medicine view of surgery
Obstructive Sleep Apnea Hypopnea Syndrome Anatomy (small, collapsible upper airway) CPAP Oral Appliance, etc. Anatomic Surgery Pharyngeal muscle activation (low gain and reflex response) Sleep (low arousal threshold) Senstivity of the ventilatory control system loop gain Decker et al 1993