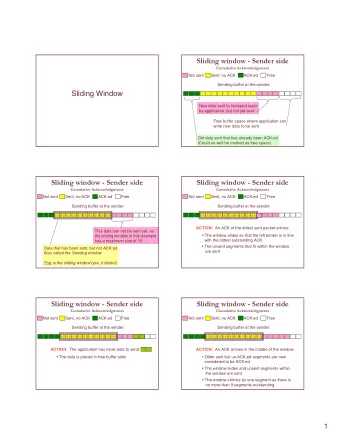
L’angor mésentérique Une pathologie méconnue CMI (Chronic Mesenteric Ischemia) Dominique Fabre, Benoit Gerardin, Delphine Mitilian, David Boulate, Carlos Garcia Alonzo, Philippe Brenot, Elie Fadel, Ramzi Ramadan, Julien Guihaire, Philippe Deleuze, Adam Bouchareb, Riyad Bourkaib Delphine Macret, Benedicte Fadel, Sacha Mussot, Olaf Mercier, Jeremy Bendavid, Antoine Girault, Justine Mougin, Stephan Haulon. Centre de chirurgie Aortique HOPITAL MARIE LANNELONGUE UNIVERSITE PARIS-SUD SACLAY
CMI (Chronic Mesenteric Ischemia) case • 70 years old men • AF • SMA stenosis • PAD Rutherford stage V • Previous EVAR • CMI
CPR 3D reconstruction
CMI / Chronic mesenteric ischemia Chronic mesenteric ischemia = rare / challenging clinical entity • Vascular patients • Most surgeons have limited experience with the management of symptomatic • occlusive disease of the superior mesenteric artery or coeliac trunk. An endovascular-first strategy : • – Less invasive character, – lower peri-procedural morbidity and mortality – more rapid recovery. Volume stenting increased • Long-term results of percutaneous mesenteric angioplasty and stenting are worse • than those obtained with open surgery. Many centres reserve open repair for cases in whom PTA failed. •
Diagnosis / CMI Chronic mesenteric ischemia (CMI) is the result of insufficient mucosal perfusion of the • gastrointestinal tract. The diagnosis of CMI is established by multidisciplinary consensus and confirmed if • successful therapy results in symptom relief. low-risk, intermediate-risk and high-risk patients for CMI. • The most common cause of isolated celiac artery (CA) stenosis is compression of the • CT by the median arcuate ligament (median arcuate ligament syndrome (MALS)).
Incidence • The exact incidence of CMI is unknown, since population-based studies are lacking. • However, the number of CMI patients undergoing revascularization procedures is increasing significantly according to data from the United States: 1.8 per million in 2000 to 5.6 per million in 2012 (p<0.01)). Zettervall SL, Lo RC, Soden PA, et al. Trends in treatment and mortality for mesenteric ischemia in the United States from 2000 to 2012. Ann Vasc Surg 2017;
What is a symptomatic patient? Haben ( Mayo clinic Experience) JVS 2019
Van Djick U Eur Gastro Ent J 2019
Van Djick U Eur Gastro Ent J 2019
CMI Score Van Djick U Eur Gastro Ent J 2019
Techniques of revascularisation • Endo • OR • ROMS: Retrograde open mesenteric stenting for acute / Chronic mesenteric ischemia
Focal / complex desease
Endo = Femoral Use steerable sheath
ROMS: Retrograde open mesenteric stenting for acute / Chronic mesenteric ischemia
Use of embolic protection device
Endo / complex case CMI after FEVAR
Through and Through wire CT / SMA
CMI after AMI • 35 y old men • PAD • claudication • Spontaneous thrombosis of the SMA / stenting BMS • Rethrombosis • CMI
Covered stent Bentley Begraft BMS / Dissection
OR Antegrade/ Retrograde
Does the early benefit and better safety profile of minimally invasive endovascular mesenteric revascularisation offset its lower long-term patency ? • For most authors, the balance between the early benefit, in terms of safety, and the late risk of reintervention after endovascular mesenteric procedures, is considered as a reasonable trade-off, favouring endovascular over open approach. ENDO > OR Alahdab A. Systematic review and meta-analysis of endovascular versus open surgical revascularization for chronic mesenteric ischemia. J Vasc Surg. 2018 Arya S. Open mesenteric interventions are equally safe as endovascular interventions and offer better midterm patency for chronic mesenteric ischemia. Ann Vasc Surg. 2016
Endo vs OR Metanalysis 100 observational studies (22 comparative, 78 noncomparative; 18,726 patients; mean age, • 69 years). OR associated with a statistically significant: • increase in the risk of in-hospital complications (relative risk [RR], 2.2; 95% confidence – interval [CI], 1.8-2.6) and Non significant increase in mortality at 30 days (RR, 1.57; 95% CI, 0.84-2.93). – lower risk of 3-year recurrence rates (RR, 0.47; 95% CI, 0.34-0.66) – similar 3-year survival. – CONCLUSIONS: EnDO may offer better early outcomes than OR • although this effect may not be durable. • Long-term mortality appears to be similar. • Alahdab A. Systematic review and meta-analysis of endovascular versus open surgical revascularization for chronic mesenteric ischemia. J Vasc Surg. 2018
Need for reinterventions • The higher need for reintervention after mesenteric artery stenting does not influence long-term survival Tallarita T, Patient survival after open and endovascular mesenteric revascularization for chronic mesenteric ischemia. J Vasc Surg. 2013
ENDO vs OR • No randomized controlled trials, • 15475 patients CMI (2000 – 2014) • Endo 70% • OR 30% • lower in-hospital mortality for ENDO: 2.4% versus 8.7% OR • shorter length of stay for ENDO: 6.4 days versus 14 days OR • lower hospitalisation cost for ENDO 21,686 $versus 42,974 $ OR ENDO advantage in better early outcome, • • OR: 7.2 odds for in-hospital mortality. Erben Y, Jean RA, Protack CD, et al. Improved mortality in treatment of patients with endovascular interventions for chronic mesenteric ischemia. J Vasc Surg. 2018.
Lima. JACC. 2017.
Endo vs OR activity Lima. JACC. 2017.
Covered stents vs BMS Covered (n1/442) vs BMS (n1/4147) 1 • superior performance of covered stents at 29-month followup, in • terms of: less restenosis (8% versus 47%), • less symptom recurrence (8% versus 50%) • less need for reintervention (9% versus 44%) • 2-year significant restenosis rate of 11% for covered compared with • 34% for bare-metal stents 2 1 Oderich G. Comparison of covered stents versus bare metal stents for treatment of chronic atherosclerotic mesenteric arterial disease. J Vasc Surg. 2013 2 Zhou Y, Outcomes of endovascular,treatments for in-stent restenosis in patients with mesenteric atherosclerotic disease. J Vasc Surg. 2019.
Flairing / Balloon intra aortic part > 2 mm CS / BMS: • higher freedom from restenosis (92% ± 6% vs 53% ± 4%; P = .003), • symptom recurrence (92 ± 4% vs 50 ± 5%; P = .003), • reintervention (91% ± 6% vs 56% ± 5%; P = .005), • better primary patency at 3 years (92% ± 6% vs 52% ± 5%; P < .003). • Secondary patency rates were similar in both groups. • CONCLUSIONS: • In this nonrandomized study, CS were associated with less restenosis, recurrences, and • reinterventions than BMS in patients undergoing primary interventions or reinterventions for CMI.
Is there any place for open surgery? • For young low-risk patients, <50 years old • OR revascularisation has authors ’ preference • Most durable vascular repair to the patient • With a 85% 10-year primary patency rate Alahdab F, A systematic review and meta-analysis of endovascular versus open surgical revascularization for chronic mesenteric ischemia. J Vasc Surg. 2018 Lejay A, Georg Y, Tartaglia E, et al. Chronic mesenteric ischemia: 20-year experience of open surgical treatment. Eur J Vasc Endovasc Surg. van Petersen AS. Open or percutaneous revascularization for chronic splanchnic syndrome. J Vasc Surg. 2010.
Should multiple mesenterial vessels be repaired (combined CT and SMA revascularisation)? • When CT and SMA are both significantly stenosed, • > 70% • it is preferable to revascularise both arteries. Lejay A. Chronic mesenteric ischemia: 20-year experience of open surgical treatment. Eur J Vasc Endovasc Surg. 2015 McAfee MK, Influence of complete revascularization on chronic mesenteric ischemia. Am J Surg. 1992 Malgor RD. Results of single- and two-vessel mesenteric artery stents for chronic mesenteric ischemia. Ann Vasc Surg. 2010
Is prophylactic intervention on asymptomatic stenosis of the mesenteric or coeliac artery justified? Resist the temptation to treat asymptomatic stenosis of the CT/ SMA often an • incidental finding on abdominal computed tomography. Splanchnic vasculature is characterised by its plasticity and rich collateral • network between the three main mesenterial vessels A solitary mesenteric artery stenosis is often well tolerated and does not • routinely requires a revascularisation procedure Oderich. Open surgical treatment for chronic mesenteric ischemia in the endovascular era: when is it necessary and what is the preferred technique? Semin Vasc Surg. 2010; Thomas JH. The clinical course of asymptomatic mesenteric arterial stenosis.J Vasc Surg. 1998.
Conclusions • CMI is not so rare and has a high mortality • A multidisciplaniry team discussion is needed to confirm the best therapeutic option • The diagnosis is offen difficult but the Score risk need to be used • Endo is the reference treatment for patients > 50 years • OR is a durable solution for patients < 50 years • Covered stents have better results than BMS
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries
![m] Sent: Wednesday, March 16, 2016 2: 27 PM To: Ali, Khadija Subject: Re: Mar 21 Thank you! Sent](https://c.sambuz.com/83814/m-s.webp)