Indigenous Population in the Americas Mexico 15.7 millions 15% - PDF document
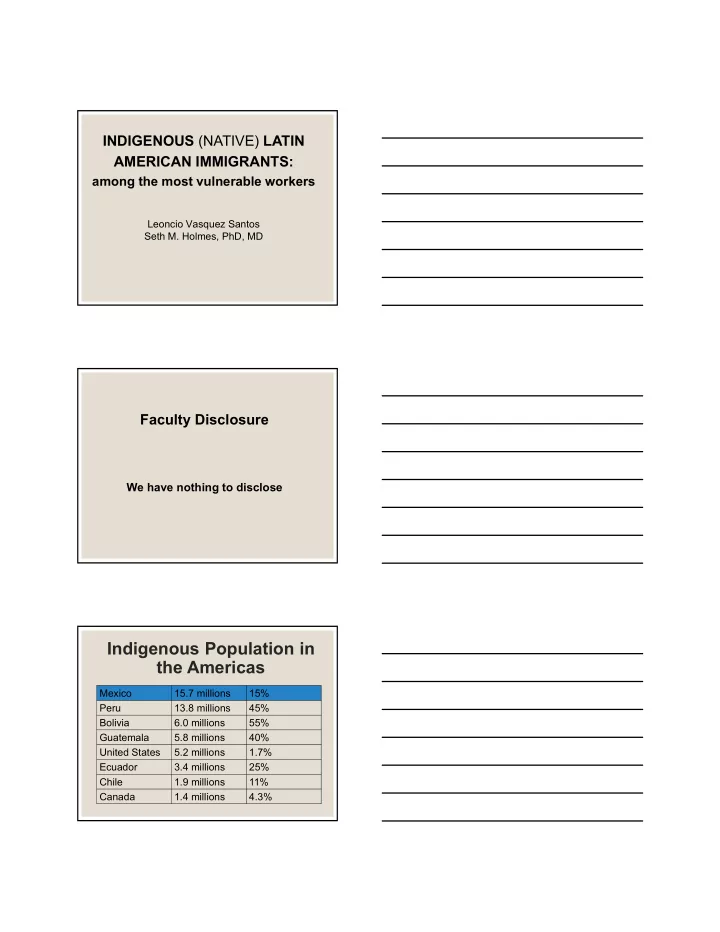
INDIGENOUS (NATIVE) LATIN AMERICAN IMMIGRANTS: among the most vulnerable workers Leoncio Vasquez Santos Seth M. Holmes, PhD, MD Faculty Disclosure We have nothing to disclose Indigenous Population in the Americas Mexico 15.7 millions 15%
INDIGENOUS (NATIVE) LATIN AMERICAN IMMIGRANTS: among the most vulnerable workers Leoncio Vasquez Santos Seth M. Holmes, PhD, MD Faculty Disclosure We have nothing to disclose Indigenous Population in the Americas Mexico 15.7 millions 15% Peru 13.8 millions 45% Bolivia 6.0 millions 55% Guatemala 5.8 millions 40% United States 5.2 millions 1.7% Ecuador 3.4 millions 25% Chile 1.9 millions 11% Canada 1.4 millions 4.3%
Indigenous Languages in Oaxaca Spanish Chontal Zapoteco Mazateco Mixteco Chinanteco Triqui Cuicateco Chatino Amusgos Serrano Huave Mixe Techuantepecano Netzichu Zoque Indigenous History The 16 ethnic communities of Oaxaca • are part of the Mesoamerican Pre- Hispanic Cultures. Social & Political Organization: • City States governed by royal o lineages Hierarchical social structure o Advance forms of art, literature, o math, cosmology Close relationship with nature o Practice of traditional medicine o Indigenous People face stigma & • discrimination even in Mexico.
Montealban Indigenous Culture • Written Language o Mixtec Codex kept 1,000 years of history o Only nine Codex remained • Oral tradition is predominant in the indigenous communities Millenary Cultural Traditions El Tequio • Offering ceremonies • to the rain God to ask for good harvest. Guelaguetza • Fiestas Patronales • Día de los Muertos • Traditional Medicine •
Indigenous Medicine Common Beliefs and Practices ● Traditional Medicine Approaches: ● Herbolaria : Use of medicinal plants/herbs. ● Midwives : Treatment during pregnancy. ● Hueseros : Treatment for bone problems ● Sobadores : Treatment for muscle pain / sprains ● Spiritual Guides : Spiritual realm of supra-natural conditions Migration to the U.S. Mexican Migration Pattern Mexico: (Always) • Veracruz • Distrito Federal • Sinaloa • Baja California Norte/Sur United States: (’80s) • California • Washington State • Oregon • Florida • New York • North Carolina
Migration to U.S. 1960s & 1970s : First indigenous families arrived with the Bracero • Program • 1980s : Begins Massive Migration o Early ’80’s: Only Men o After IRCA (1986): Increased in the number of whole families • 1990 : U.S. Census registers one Mixtec family • 1991 : The California Institute for Rural Studies conducted a research and found that 50,000 indigenous migrants worked in the fields of California. 2008-2009 : The “Indigenous Farmworker Study” estimates that • number of indigenous persons working in the agriculture sector in California is 120,000 and it reaches 165,000 when children are included. (Mines et al., 2010) Estimate: 120,000 in CA Farmworker Families + 45,000 Children Challenges Facing Indigenous Migrants Racial Hierarchy • Racism & Prejudice (stereotypes) • “No seas indio!” Class Exploitation • Worse paid jobs for newcomers • “They like to work bent over.” Cultural and Language Barriers • Language not dialect • The glorious past vs. the harsh present • The politics of cultural difference
Conditions of Indigenous Migrants in the U.S. They perform the most physical • demanded and less rewarded jobs (farm work and construction) They are exposed to pesticides, o long working hours, no toilets with water to wash hands and drinking water. • They earn the minimum wage and too often below the minimum wage Zabin and others (1993) found that • Mixtec workers were more likely to accept jobs paying less than the minimum wage and were more likely to be victims of non-payment and other law violations. Living Conditions Living Conditions • It is common to find two bedroom apartments with two or three families (15 people). • Many live in caves, around the rivers, mountains and under the orchard trees.
Living Conditions Living and Working Conditions Immigration, Identity and Social Networks • Informal Village Networks • Formalization of Social Networks. • Institutionalization of collective practices (political, social, economic and religious). • Emergence of a subjective collective belief of membership and belonging.
Structural Competency “A shift in medical education … toward attention to forces that influence health outcomes at levels above individual interactions.” –Metzl and Hansen 2014 The capacity for health professionals to recognize and respond to health and illness as the downstream effects of broad social, political, and economic structures. Structural Competency Develop trainees’ capacity in: 1. Recognizing the influences of structures on patient health 2. Recognizing the influences of structures on the clinical encounter 3. Responding to the influences of structures in the clinic 4. Responding to the influences of structures beyond the clinic 5. Structural humility Social Structures ● The policies, economic systems, and other institutions (judicial system, schools, etc.) that have produced and maintain contemporary social inequities and health disparities, often along the lines of social categories such as race, class, gender, and sexuality.
Structural Violence ● “Structural violence is one way of describing social arrangements that put individuals and populations in harm’s way... The arrangements are structural because they are embedded in the political and economic organization of our social world; they are violent because they cause injury to people.” – Farmer et al. 2006 Structural Vulnerability ● The risk that an individual experiences as a result of structural violence – including their location in multiple socioeconomic hierarchies. Structural vulnerability is not caused by, nor can it be repaired solely by, individual agency or behaviors.
Metzl and Roberts, “We argue that, if stigmas are not primarily produced in individual encounters but are enacted there due to structural causes, it then follows that clinical training must shift its gaze from an exclusive focus on the individual encounter to include the organization of institutions and policies, as well as of neighborhoods and cities , if clinicians are to impact stigma-related health inequalities.”
Research shows: • SC is effective in shifting student perceptions of disease etiology o Before SC Training: genetics, behavior, culture o Post-SC Training: poverty, racism, harmful policies, unequal resources • Trainees indicate increased empathy and solidarity with patients Case One “Mr. Martinez is a 28 year-old male found down and intoxicated, possible aspiration pneumonia. He's a frequent flyer with many similar presentations but no history of alcohol withdrawal seizures. Nothing to do. If he's agitated assess for withdrawal and start the withdrawal protocol.” I n E me rg e nc y Be g ins Drinking De pa rtme nt Afte r Ge ts Assa ulte d Mo re He a vily F o und o n the Stre e t Standar d Me dic al History & De fault Provide r Inte rpre tation Be g ins Wo rking I njury, Ca n’ t Pa y Re nt, a s Da y L a b o re r Ca n’ t Wo rk Mo ve s to Stre e t 4 th Ge ne ra tio n I nflux o f Che a p US Mo ve s to Sa n Co rn; Ca n’ t Ma ke Co rn F a rme r in F ra nc isc o a L iving Oa xa c a
I n E me rg e nc y Be g ins Drinking De pa rtme nt Afte r Ge ts Assa ulte d Mo re He a vily F o und o n the Stre e t City polic ie s Punitive US immigration c ontributing to high Polic y/ Disc rimination re nts & displac e me nt Syste matic Be g ins Wo rking I njury, Ca n’ t Pa y Re nt, marginalization of a s Da y L a b o re r Ca n’ t Wo rk Mo ve s to Stre e t and viole nc e against indige nous Nor th Ame r ic an F r e e c ommunitie s in Rac ialize d low-wage T rade Agre e me nt S. Me xic o labor marke ts No He alth Insuranc e (NAF T A) (e xc lude d fr om ACA) 4 th Ge ne ra tio n I nflux o f Che a p US Mo ve s to Sa n Co rn; Ca n’ t Ma ke a Co rn F a rme r in F ra nc isc o L iving Oa xa c a I n E me rg e nc y Be g ins Drinking De pa rtme nt Afte r Ge ts Assa ulte d Mo re He a vily F o und o n the Stre e t Standar d Me dic al History & De fault Provide r Inte rpre tation Be g ins Wo rking I njury, Ca n’ t Pa y Re nt, a s Da y L a b o re r Ca n’ t Wo rk Mo ve s to Stre e t 4 th Ge ne ra tio n I nflux o f Che a p US Mo ve s to Sa n Co rn; Ca n’ t Ma ke a Co rn F a rme r in F ra nc isc o L iving Oa xa c a Naturalizing Inequality • The sometimes subtle, sometimes explicit, ways in which structural violence is erased and elided by claims of cultural difference, genetic variance, behavioral shortcomings, or racial categories. • “Noncompliant” “Lost to follow-up” “Frequent flyer” • The “Culture of Poverty” (usually poor communities of color) • “Risk factors” as decontextualized, objective, apolitical realities
Recommend








More recommend
Explore More Topics
Stay informed with curated content and fresh updates.