Illicit Drug Use in Pregnancy I have the following relationship: - PowerPoint PPT Presentation
Disclosures Illicit Drug Use in Pregnancy I have the following relationship: Deirdre Lyell, MD Bloom Technologies - Advisor Professor, Obstetrics and Gynecology Program Director, MFM Fellowship Director, Program in Placental Disorders
Disclosures Illicit Drug Use in Pregnancy � I have the following relationship: Deirdre Lyell, MD Bloom Technologies - Advisor Professor, Obstetrics and Gynecology Program Director, MFM Fellowship Director, Program in Placental Disorders Stanford University Medical Center UCSF AIM Conference I have no disclosures related to the content June 9, 2016 of this presentation Objectives Why this topic? � Overview of: � Obstetric providers: � current patterns of drug use and specific issues � Screen, diagnose, educate, counsel, initiate treatment � pregnancy morbidities of specific drugs • Marijuana, opiates/methadone � neonatal abstinence syndrome (NAS) � Time of increased motivation � screening � Pregnancy-related abstinence among users: 57% � breastfeeding � Resumption of use first year after pregnancy is lower � anesthetic issues, pearls than that of non-new mothers
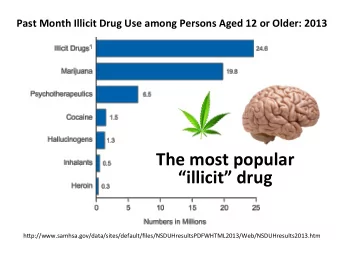
What is the most frequently used What is the second most frequently illicit drug in the U.S.? used illicit drug in the U.S.? A. Prescription pain relievers A. Prescription pain relievers B. Hallucinogens B. Hallucinogens 60% 97% C. Cocaine C. Cocaine 39% D. Marijuana D. Marijuana 1% 1% 1% 0% 0% e a e a s s s s r n n n r n n n e e e a i a e a i a v g u v g u c c e o o j e o o j i i i i l n C r l n C r e i a e i a c M c M r u r u n n l l i l i l a a a a p H p H n n o o i i t t p p i i r r c c s s e e r r P P Drugs of Choice in U.S. Patterns of use in U.S. (2012-2013) � Survey of 67,500 people 12+ years old: � Ages 15-44: 5.4% of pregnant women used illicit drugs in the last month (versus 11.4% 1 st Marijuana non-pregnant) 2 nd Psychotherapeutics: non-medical use of pain killers � 15-17 years: 14.6% then tranquilizers, stimulants and sedatives 3 rd Cocaine � 18-25 years: 8.6% 4 th Hallucinogens � 26-44 years: 3.2% � Poly-substance use common � Not significantly different from 2010-2011 Substance Abuse and Mental Health Services Administration. Result from the 2013 National Survey on Drug Use and Health: Summary of National Findings, NSDUH Series H-48, HHS Publication 14-4863, 2014 Substance Abuse and Mental Health Services Administration, Results from the 2013 National Survey on Drug Use and Health; 2014
Opiate use is increasing � 2000: 1.19/1000 births (95% CI 1.01-1.35) Pregnancy Morbidities of Specific Drugs � 2009: 5.63/1000 births (95% CI 4.40-6.71) Does marijuana cross the Limitations of data placenta? � Multiple confounding variables � Polypharmacy frequent 89% A. Yes • Other drugs, alcohol, tobacco B. No � Poor social circumstances, poverty, late to care or inadequate care, poor nutrition, co-morbidities � Incomplete testing/reporting, scarce data 11% � No prospective studies s o e N Y
Marijuana Marijuana � Tetrahydrocannabinol (THC) � Most frequent illicit drug in pregnancy � Small, highly lipophilic molecule, distributes rapidly to brain and fat � Prevalence (2-5% overall) increases to � Half-life varies: 30% among urban, socioeconomically � 20-36 hours in occasional users � 4-5 days in heavy users disadvantaged young women � Can take 30 days for complete excretion � Approximately 50% continue use during � Crosses the placenta pregnancy � Fetal levels in mouse are initially 10% of ingested levels � Belief that it is relatively safe � Higher concentrations seen with repetitive use � Less expensive than tobacco � Current products have higher THC content than past Marijuana Marijuana � Prospective cohort study, n=5588 nulliparous, low-risk � No high-quality data to suggest teratogenic women (SCOPE study), 90%Caucasian effect � Self-reported marijuana and tobacco use � Embryotoxic in rabbits � Adjusted for maternal age, tobacco, alcohol, SES � Continued marijuana use at 20 weeks associated with: � Several small studies suggest increased low � 5.4 fold increased spontaneous preterm birth (sPTB; birth weight, preterm birth, SGA and NICU 95% CI 2.44-12.11) • 11 women: 4 (36%) delivered <28 weeks; 7 <32 weeks (64%) admission � Dose-dependent effect � Many confounding variables � Effect not seen for women who quit <20 weeks • Saurel-Cubizolles et al, BJOG 2014; � No differences in SGA, preeclampsia Hayatbakhsh et al, Pediatr Res � Authors estimated cessation of marijuana would result in 2012;71:215 6.2% reduction in sPTB Leemaqz SY et al, Reproductive Toxicology 62(2016)77-86 � Delayed motor development at 1 year
How many hours since last use do Opiates heroin withdrawal symptoms peak � Not teratogenic A. 12 hours � Risks: social and withdrawal 33% B. 16 hours � Obstetric issues are difficult to separate from withdrawal, polypharmacy, social issues and C. 24 hours 25% other confounding variables D. 48 hours � Multiple problems in pregnancy: 16% � Spontaneous abortion, IUGR, stillbirth, intra- E. 60 hours 13% 13% amniotic infection, abruption, preeclampsia, preterm labor and delivery, PPROM, placental insufficiency, postpartum hemorrhage, septic pelvic thrombophlebitis s s s s s r r r r r u u u u u o o o o o h h h h h 2 6 4 8 0 1 1 2 4 6 Heroin withdrawal Risks of withdrawal � Maternal: relapse, increased drug seeking behaviors � Fetal withdrawal (intrauterine abstinence syndrome, IAS): • “ A high percentage of mothers who are detoxified revert back to Rementeria et al., 1973 (AJOG): term stillbirth following narcotic � withdrawal than ‘withdraw’ the addict during pregnancy? ” heroin….wiser to encourage methadone programs to ‘maintain’ rather Zuspan et al., 1975: elevated amniotic fluid epinephrine levels during � methadone detox despite normal maternal catecholamine levels, improved with increased methadone dose Wang W et al., 1997, Case report of withdrawal in 29 week EGA with � IUGR and AEDF. Dopplers returned to normal after administration of methadone • Suggests withdrawal can reversibly affect fetal placental circulation
Opiates: substitution therapy recommended � Preferable to withdrawal: safe, lower rate of resumption of heroin Neonatal Abstinence � Methadone or buprenorphine � Oral administration, known dose, available, improved Syndrome (NAS) maternal/fetal/neonatal outcomes � Methadone shown to: � increase fetal weight � improve compliance with prenatal care � reduce exposure to illicit substances � potentially improve custody retention rates due to less frequent relapse Cochrane Reviews, 2008; Messinger Pediatrics 2004 � � Emphasizes importance of stabilizing the home for child development � At 3 years old, no difference in outcomes after corrected for confounding social factors What is NAS? What is NAS? � Excessive or continuous high pitched crying � Array of newborn signs and symptoms after � Sleeps less than 1 hour after feeds birth in the setting of fetal drug exposure � Hyperactive Moro reflex (typically opioids: heroin, methadone, � Tremors, myoclonic jerks, generalized seizures hydrocodone [vicodin], oxycodone [oxycontin]) � Withdrawal signs: sweating, frequent yawning, moaning, nasal stuffiness, sneezing, nasal flaring, tachypnea, excessive sucking, poor feeding, � Often seen at 24-48 hours, may be delayed as regurgitation, vomiting, loose or watery stools, fever long as 10 days � Treatment: first supportive with IV fluids, extra � Akin to CNS overstimulation calories, comfort; if more severe, pharmacotherapy (oral morphine or methadone) with wean https://www.drugabuse.gov/publications/research-reports/substance- https://www.drugabuse.gov/publications/research-reports/substance-use-in-women/substance- use-in-women/substance-use-while-pregnant-breastfeeding use-while-pregnant-breastfeeding NIH: National Institute on Drug Abuse NIH: National Institute on Drug Abuse
Methadone dose not predictive of Scope and cost of NAS NAS severity � Retrospective review, 100 mother/infant pairs on � Increasing with increasing opiate use methadone � <80 mg versus >80 mg � Among 650,000 neonates born in U.S. 2004-2013 � No difference in highest NAS score, need for or length of treatment � NAS increased from 7 cases/1000 NICU � More illicit use if <80 mg admissions to 27 cases/1000 � Berghella V et al, AJOG 2003 • 3.86-fold increase � Retrospective review of 81 mother/infant pairs on � Total NICU days for NAS increased from 0.6% methadone � <100 mg versus >100 mg to 4.0% � No differences in need for treatment of NAS or length of • Tolvia VN et al., NEJM 2015 stay � More illicit substance abuse at delivery if <100 mg � McCarthy JJ et al, AJOG 2005 � 42-94% infants of opiate abusers experience NAS � Higher methadone doses may decrease illicit drug use � In 2011: $750,000,000 in NICU charges (US) and high risk behaviors Stanford Study: Prevention of NAS Protocol � Ondansetron reduces opiate withdrawal in adults and animals � Study sites: Stanford, UCSF, SCVMC, University of Utah, Johns Hopkins University � Double-blind, placebo controlled, randomized study of 90 neonates born to 90 opioid-dependent mothers � NIH/NICHD R01-funded study, PI David � Inclusion: pregnant women 18-45 years, Drover, MD singletons, term (37 to <42 weeks), opioids for at least 3 weeks prior to delivery, vaginal delivery or � Research coordinator: cesarean � Carol Cohane, RN, 650-736-8231 � Ondansetron � cohane@stanford.edu � If possible: I.V. at least 30 minutes prior to delivery � Newborn: oral or I.V. ondansetron qD x 5 days, beginning 4-8 hours of life � Primary outcome: incidence NAS
Recommend








More recommend
Explore More Topics
Stay informed with curated content and fresh updates.