If not us, who? The case for treating addiction in primary care September 2019 Community Care Network of Kansas Annual Conference Kelly.Pfeifer@dhcs.ca.gov
Disclosures: • I never received money from pharma. I am not representing the State of California. • • I spent the first 5 years of my career fueling the opioid epidemic.
Beth Name and picture changed
The cause was clear… we made a plan.
California, 2015-2018: Dramatic drop in opioid prescribing
It’s not just opioids Credit: Matt Willis, MD MPH
We won’t stop the deaths until we change how we think about addiction
We need three things to survive: food, water and dopamine R Corey Waller, MD How opioids change the brain https://www.youtube.com/watch?v=bwZcPwlRRcc California Health Care Foundation www.chcf.org 12
Dopamine changes over time 13 9/9/2019 California Health Care Foundation www.chcf.org 13
Addiction is a brain disease: living in a tempest
Medicatio ion c calms t the brain in, f facilit litates p partic icip ipatio ion i in beha havioral h health a h and s d social s suppo pport, a and a d allows r recovery • Methadone: cuts death rates by 67% • Buprenorphine: cuts death rates by 50% • Naltrexone: works for some populations; no impact on death rates in large, long- term trials Detox then drug-free tx : 2-3x death rates compared to maintenance Sordo et al., Mortality risk during and after opioid substitution treatment: systematic review and meta-analysis of cohort studies, BMJ 2017; 357;j1550; Larochelle, California Health Care Foundation www.chcf.org 15 et al. Ann Intern Med. 2018;169(3):137-145; DOI: 10.7326/M17-3107
So how do we build a bigger boat?
AIDS Deaths, United States: 1981-1995 • 1995: 55,000 AIDS deaths • Continuous rise over prior decade 1995: 55,000 AIDS deaths Source: Centers for Disease Control, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention 17 9/9/2019
Primary care Responses to HIV in the ‘90s “These patients are too “These patients are too disruptive for our practice.” complex– we don’t have the clinical expertise.” “They brought this on “We’re just one part of the themselves. They knew the system. We can’t do this risks and made their choices.” alone.”
HIV now Ubiquitous routine screening Treatment access widespread Almost normal life expectancy
What can HIV teach us about bigger boats?
Lessons from HIV 1. Screen widely 2. Make treatment easy to find: no wrong door 3. Stop the stigma 4. Promote harm reduction 5. Don’t do it alone 6. Tackle racism
Lessons from HIV 1. Screen widely 2. Make treatment easy to find: no wrong door 3. Stop the stigma 4. Promote harm reduction 5. Don’t do it alone 6. Tackle racism
Screen widely: We can’t help if we don’t know. We won’t know if we don’t ask. Support evidence; support MAT.
Lessons from HIV 1. Screen widely 2. Make treatment easy to find: no wrong door 3. Stop the stigma 4. Promote harm reduction 5. Don’t do it alone 6. Tackle racism
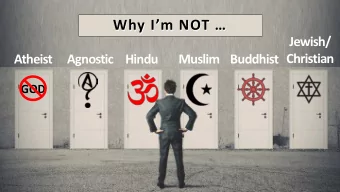
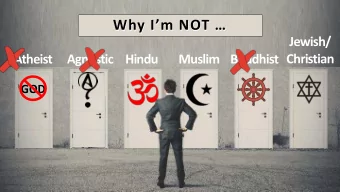
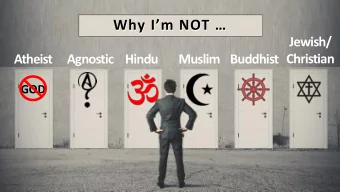
NOT < California Health Care Foundation www.chcf.org 26
Make treatment easy to find. No wrong door. • Treat the disease, not the symptom • Train and support clinicians • If you can’t integrate, coordinate • Step-up and step-down care (like any other chronic disease)
Treatment s starts her here: e: MAT a at e ever ery hea health c care t e touc uchpoint
Lessons from HIV 1. Screen widely 2. Make treatment easy to find: no wrong door 3. Stop the stigma 4. Promote harm reduction 5. Don’t do it alone 6. Tackle racism
Stop the stigma
Patients need help combatting stigma: friends, family, 12-step groups, treatment centers…
Words can heal; words can harm We need to replace this: With this:
Lessons from HIV 1. Screen widely 2. Make treatment easy to find: no wrong door 3. Stop the stigma 4. Promote harm reduction 5. Don’t do it alone 6. Tackle racism
Promote Harm Reduction • Risky behavior won’t go away Some behaviors are safer than • others • Our goal is improved life for people and communities • We should help minimize harm
We are good with harm reduction – for diabetes. Cause? Genes, environment, and behavior Prevention? Environmental and behavior change Treatment? Long-term chemical replacement; lifestyle changes Noncompliance: Support small changes. Keep treating.
Yes Diabetes vs. Addiction: what can you lose? Treatment No Yes No Yes Custody of children Freedom (probation) No Yes The list goes on.. housing, family, work, and more
The cost of expecting perfection People cut off opioid pain meds are twice as likely to use illicit drugs Veterans: higher risk of suicide and mental health crisis when opioids tapered to zero Half of people discontinued off opioids were stopped abruptly; half of those were admitted to the ED or hospital for opioid-related diagnoses. Pre-publication from Phillip Coffin’s study of tapering outcomes. Demidenko, M., et al, Suicidal ideation and suicidal self-directed violence following clinician-initiated prescription opioid discontinuation among long-term opioid users, Gen Hosp Psychiatry 2017 Jul; 47:29-35, https://www.ncbi.nlm.nih.gov/pubmed/28807135 http://www.bmj.com/content/357/bmj.j1550
Lessons from HIV 1. Screen widely 2. Make treatment easy to find: no wrong door 3. Stop the stigma 4. Promote harm reduction 5. Don’t do it alone 6. Tackle racism
Don’t do it alone • Warmline: free addiction specialist expertise to help you with cases and commonly asked questions • Resources: SAMHSA, Provider’s Clinical Support System (PCSS-MAT), CHCF • Relationship with opioid treatment program (step-up and step-down) • Telehealth: direct to patient, e-consultation, or shared management
Telepsychiatry providers adding MAT Telehealth providers specializing in MAT https://www.chcf.org/publication/innovation-landscape-telehealth-mat/
www.chcf.org
Levels of care: primary care MAT Hire addiction counselors and/or peers. Train staff and clinicians in management of other SUDs. Contract with counties and plans as SUD treatment provider. Level 3 Train staff in SBIRT screening. Train behavioral staff in motivational interviewing for SUD. Have MA do check-in calls during buprenorphine starts. Do buprenorphine group visits, co-led by clinician and Level 2 behaviorist. 2 clinicians get a waiver. Level 1 Treat simple OUD; transfer complex patients (persistent + drug screens) to opioid treatment program. Accept bupe maintenance patients. Transition high-dose pain patients onto bupe
HIV care got a bigger boat. What happened?
AIDS deaths: 1981-2007 Widespread screening Access to effective treatment Anti-stigma campaign Harm reduction Team care --- AIDS deaths Source: Centers for Disease Control, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention
The French Experience: 80% Drop in Deaths Heroin OD deaths Buprenorphine prescriptions Methadone treatment
Why not zero? --- AIDS deaths Source: Centers for Disease Control, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention
Lessons from HIV 1. Screen widely 2. Make treatment easy to find: no wrong door 3. Stop the stigma 4. Promote harm reduction 5. Don’t do it alone 6. Tackle racism
https://www.youtube.com/watch?v=-4YDUDhMcvM Apologies in advance: it is impossible to beep out profanity from Wanda
Lessons from HIV 1. Screen widely 2. Make treatment easy to find: no wrong door 3. Stop the stigma 4. Promote harm reduction 5. Don’t do it alone 6. Tackle racism Level 3 Start simple. But start now. Level 2 Level 1
Helping people recover can support our own recovery. Rediscover the joy of medicine. If not us, who? Kelly.Pfeifer@dhcs.ca.gov
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries