How Potential Changes to Medicare’s Buy-and-Bill Model May Affect Your Hub John Carlsen Vice President, Market Access Consulting February 2019 Important Disclaimer: According to the Trump administration’s spring 2019 regulatory agenda released on May 22, 2019, the proposed rule on the International Pricing Index (IPI) Model for Part B Drugs has been delayed until August 2019. The content of this presentation was developed for a conference in February 2019, and does not reflect the delayed timing of the proposed rule.
Agenda Overview of the IPI Model 1 Historical Context 2 What Happens Next? 3 Implications for Hubs 4 2
Overview of the IPI Model
International Price Index (IPI) Model for Part B Drugs October 25, 2018 Spring 2020 - Spring 2025 The Centers for Medicare and The IPI Model would test changes Medicaid Services (CMS) announced related to reimbursement for Part a potential new model for Medicare B drugs over a five-year period Part B drugs Medicare payment rates based on • Would apply to injectable/infused drugs prices in other countries administered in a physician’s office or Three Flat “add-on” payment not tied hospital outpatient department (HOPD) components to cost of drug of the Model Providers obtain drugs from private-sector vendors instead of “buying and billing” This presentation focuses on the third component of the model (a form of “white bagging”) Important Disclaimer: According to the Trump administration’s spring 2019 regulatory agenda released on May 22, 2019, the proposed rule on the IPI Model has been delayed until August 2019. The content of this presentation was developed for a conference in February 2019, and does not reflect the delayed 4 timing of the proposed rule.
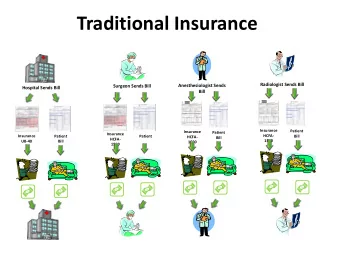
Traditional Buying and Billing under Medicare Part B Wholesaler/ Distributor “Buy” Provider (physician office or HOPD) purchases drug Provider “Bill” Bills Medicare Collects patient cost- for drug and sharing for drug and Provider bills Medicare for drug and collects admin service admin service cost-sharing from patient (or secondary insurer); also bills and collects cost-sharing for administration service Under this system, providers are reimbursed for most drugs at average sales price (ASP) + 6% 5
Drug Procurement and Reimbursement under the IPI Model Wholesaler/ Distributor Procurement Model vendor (e.g., specialty pharmacy) purchases drug and ships to provider Model Provider Vendor Reimbursement Collects patient cost- Bills Medicare Bills Medicare ► Model vendor bills Medicare for drug sharing for drug and for admin service for drug admin service ► Provider bills Medicare for administration service and collects cost-sharing from patient (or secondary insurer); also collects cost-sharing for drug Under this model, providers would receive no reimbursement for the drug itself , but would receive a flat add-on payment (not based on ASP) 6
Key Aspects of the IPI Model: Vendors Private-sector vendors would: • Contract with CMS to supply providers with drugs included in the model • Operate on a national basis • Negotiate drug prices with manufacturers • Take on the financial risk of purchasing drugs and billing Medicare • Be reimbursed for drugs at rates tied to international prices CMS anticipates that a variety of entities could potentially serve as vendors: • Specialty pharmacies • Group purchasing organizations (GPOs) • Wholesalers • Distributors • Part D sponsors • Physicians and hospitals • Manufacturers • Others 7
Key Aspects of the IPI Model: Providers Providers would: • Be removed from the buying-and-billing process for included drugs • Obtain included drugs from model vendor(s) • Bill Medicare for the administration service (e.g., IV infusion) • Receive a flat add-on payment for an administered drug • Collect cost-sharing from the patient for both the drug and the administration service • Continue to buy and bill for drugs excluded from the model Providers subject to the model would include: • Physician practices • HOPDs • Potentially others (e.g., ASCs, DME suppliers) 8
Key Aspects of the IPI Model: Geographic Scope Model would be implemented in approximately half of the country • Randomized design across the U.S. • Geographic areas to be determined • Mandatory participation for providers in the geographic areas • Providers outside of the geographic areas would continue to buy and bill CMS is considering using Core Based Statistical Areas (CBSAs) for the geographic areas in the model • > 900 CBSAs in the U.S. However, CMS also notes that it may be necessary to use larger geographic areas “to avoid the potential for routine shifts in the site of care” 9
Key Aspects of the IPI Model: Included Drugs Model would initially focus on single-source drugs and biologicals (including biosimilars): • Included drugs would need to have sufficient international pricing data • At a minimum, CMS expects to begin the model by including “most” of the 32 “top Part B drugs” referenced in a recent HHS report* • Would also include multiple source drugs with a single manufacturer (and potentially other multiple source drugs) • More drugs would be added to the model over time • To-be-determined mechanism for adding newly approved drugs Certain types of drugs would be excluded from the model: • “Not otherwise classified” (NOC) drugs (e.g., J3490) • Radiopharmaceuticals • End-stage renal disease (ESRD) drugs • “Short supply” drugs as identified by the FDA • Hospital outpatient packaged drugs * U.S. Department of Health and Human Services (HHS). Comparison of U.S. and International Prices for Top Medicare Part B Drugs by Total Expenditures. October 25, 2018. Available at: https://aspe.hhs.gov/system/files/pdf/259996/ComparisonUSInternationalPricesTopSpendingPartBDrugs.pdf 10
Historical Context
Competitive Acquisition Program (CAP) for Part B Drugs July 1, 2006 – December 31, 2008 2003 January 1, 2009 White bagging program Program in operation Contractual issues established by the with bidders led CMS Medicare Modernization to indefinitely suspend Only one vendor (BioScrip) Act (MMA) as an alternative the CAP Small percentage of to the ASP methodology physicians participated, with significant attrition each • Drugs supplied by CAP Was not year vendor considered Did not achieve cost a success • Physicians removed savings from buying-and-billing Extensive logistical and process administrative requirements limited appeal of program 12
How is the IPI Model different from the CAP? CAP (2006-2008) IPI Model (target: 2020-2025) Provider participation Voluntary Mandatory Physician offices and HOPDs Provider types Physician offices (potentially others) Vendor types Specialty pharmacies only Various Allowed to select only one Can receive drugs from multiple Provider choice vendor vendors, change vendors Subject to rigid requirements Flexible arrangements permitted Drug procurement (e.g., patient-specific order (e.g., vendors not required to take required for each drug shipped) physical possession of drugs) Add-on payment None Flat rate Mandated by statute Test model CMS authority for program (MMA) (CMS Innovation Center) Important Disclaimer: According to the Trump administration’s spring 2019 regulatory agenda released on May 22, 2019, the proposed rule on the IPI Model has been delayed until August 2019. The content of this presentation was developed for a conference in February 2019, and does not reflect the delayed 13 timing of the proposed rule.
What Happens Next?
Several things must happen for the IPI Model to become a reality ► So far, CMS has only issued an advance notice of proposed rulemaking (ANPRM) ► The model still must go through the full rulemaking process: • CMS issues proposed rule (target timeframe: spring 2019) • Stakeholders submit comments on proposed rule • CMS issues final rule (late 2019?) • Model takes effect (target timeframe: spring 2020) ► Other important milestones for model implementation: • Interested vendors submit applications to CMS • CMS selects vendors • Vendors contract with CMS • Providers enroll with vendors A delay to any of the individual milestones could affect CMS’s ability to meet its target timeframe Important Disclaimer: According to the Trump administration’s spring 2019 regulatory agenda released on May 22, 2019, the proposed rule on the IPI Model has been delayed until August 2019. The content of this presentation was developed for a conference in February 2019, and does not reflect the delayed 15 timing of the proposed rule.
Many policy and operational aspects of the model still need to be determined Other important questions: Future rulemaking should provide more details on: How will exceptions be handled ► (e.g., in emergency situations)? How geographic areas will be ► What will be the rules surrounding ► defined wastage? Nature of the drug add-on payment ► How much oversight will there be ► (e.g., amount, frequency) from CMS? Specific drugs included in the model ► How will CMS match vendor and ► Process for adding new drugs ► provider claims? Coding and billing requirements ► How will the model work for large ► provider organizations that span multiple geographic areas? 16
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries