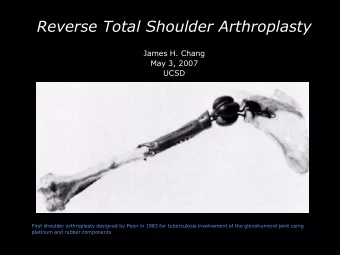
Glenoid Exposure Tips and Tricks to Achieve Reproducible Glenoid - PowerPoint PPT Presentation
Glenoid Exposure Tips and Tricks to Achieve Reproducible Glenoid Access John W. Sperling, MD, MBA Mayo Clinic Disclosure Zimmer-Biomet: Royalties Positioning Beach chair position Waist 45 , knees 30 Slightly roll the
Glenoid Exposure Tips and Tricks to Achieve Reproducible Glenoid Access John W. Sperling, MD, MBA Mayo Clinic
Disclosure • Zimmer-Biomet: Royalties
Positioning • Beach chair position –Waist 45 ° , knees 30 ° –Slightly roll the body away from the operative shoulder –Place a rolled up towel under the medial border of the scapula
Positioning
Approach • Landmarks –Posterior spine of the scapula –Lateral/Anterior border of the acromion –Clavicle –Coracoid
Approach • Incision –Begins at the anterior portion of the clavicle –Passes approximately ½ cm lateral to the coracoid
Approach • Incision –Develop the deltopectoral interval proximally – Small triangle of fat is usually present identifying the infraclavicular triangle –Vein is left medially
Deltoid Mobilization
Incise Interval-Subscapularis • Identify the rotator interval • Significant surgeon variability in technique of releasing the subscapularis – Intra-tendinous – Off bone – Osteotomy
Marking Stitches
Inferior Capsule • Inferior capsule release: stay on bone and directly visualize the capsule • Arm externally rotated and adducted, continue the release to the 4 o’clock position
Open the Door
Complete Inferior Release
Humeral Head Cut • Use a drill to gain access to humeral canal • Prepare humeral canal with hand reaming
Entry Hole
Ice Pick
Reamer
Humeral Head Cut • Cutting block is 1 mm above RC insertion • 30-35 ° retroversion is average
Humeral Guide
Head Cut
Humeral Preparation • Seat broach • Trim away metaphyseal bone
Complete Osteophyte Removal
Glenoid Exposure • Common reasons for difficult exposure –Lack of deltoid mobilization –Insufficient capsular release –Too high a head cut –Insufficient humeral osteophyte removal
Retractors
Glenoid Exposure
Glenoid Exposure
Glenoid
Glenoid
Glenoid
Glenoid
Glenoid
PSI
PSI
PSI
Summary • Key to glenoid exposure is the humeral side • When in doubt-repeat the 4 key steps – Aggressive humeral head cut – Humeral osteophyte removal – Inferior capsule – Deltoid mobilization
Thank You
Recommend






More recommend
Explore More Topics
Stay informed with curated content and fresh updates.