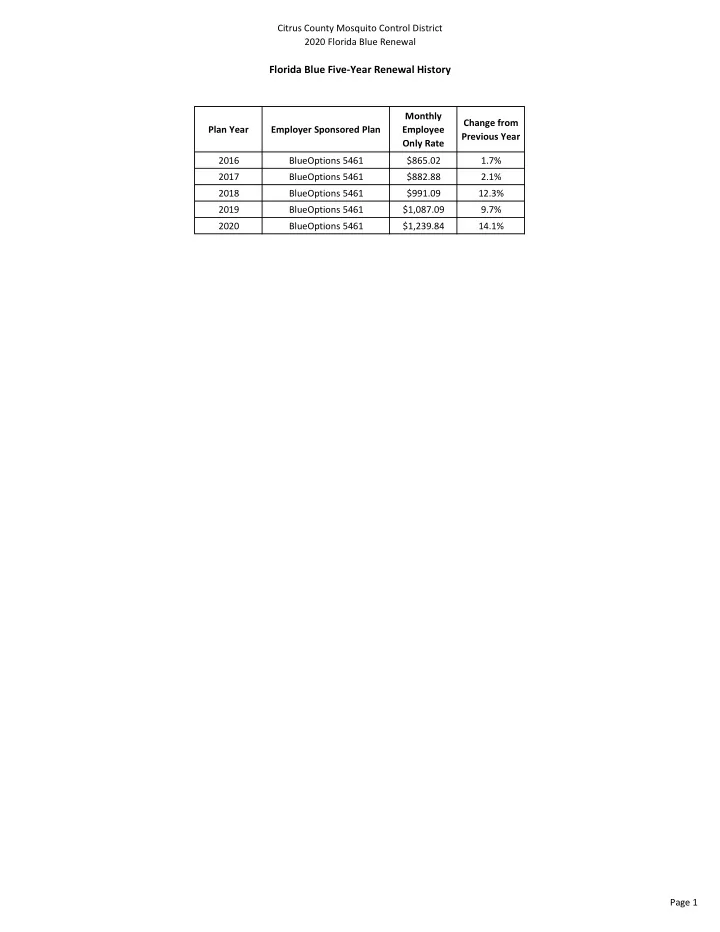
Citrus County Mosquito Control District 2020 Florida Blue Renewal Florida Blue Five-Year Renewal History Monthly Change from Plan Year Employer Sponsored Plan Employee Previous Year Only Rate 2016 BlueOptions 5461 $865.02 1.7% 2017 BlueOptions 5461 $882.88 2.1% 2018 BlueOptions 5461 $991.09 12.3% 2019 BlueOptions 5461 $1,087.09 9.7% 2020 BlueOptions 5461 $1,239.84 14.1% Page 1
Citrus County Mosquito Control District 2020 Florida Blue Renewal Renewal Summary PLAN N A PLAN N B PLAN N C BlueOptions BlueOptions BlueOptions Predictable Cost 5461 HSA-Compatible 5070/5071 HSA-Compatible 5022/5023 Deductible (per person/family) In-Network $250/$750 $3,500/$7,000 $2,500/$5,000 Out-of-Network $1,000/$3,000 $7,000/$14,000 $5,000/$10,000 Coinsurance (amount member pays) In-Network 10% 0% 20% Out-of-Network 50% 20% 40% Wellness (Routine Exam, Well Woman Exam, Family Physician $0 $0 $0 Mammogram, Well Child) Specialist $0 $0 $0 Out-of-Network Coinsurance Coinsurance Coinsurance Physician Office Services Family Physician $10 CYD CYD + 20% Specialist $25 CYD CYD + 20% CYD 1 + 50% Out-of-Network CYD + 20% CYD + 40% Inpatient Hospital Facility (per admission) Option 1 $250 CYD CYD + 20% Option 2 $375 CYD CYD + 20% Out-of-Network CYD + 50% CYD + 20% CYD + 40% ER Facility (waived if admitted) In-Network $100 CYD CYD + 20% Out-of-Network $100 CYD + 20% CYD + 40% Outpatient Hospital Facility Option 1 $100 CYD CYD + 20% Option 2 $150 CYD CYD + 20% Out-of-Network CYD + 50% CYD + 20% CYD + 40% Provider Services at Hospital & ER $50 CYD CYD + 20% Independent Diagnostic Testing Facility In-Network $50 CYD CYD + 20% Advanced 2 $75 CYD CYD + 20% Out-of-Network CYD + 50% CYD + 20% CYD + 40% Independent Clinical Lab In-Network $0 CYD CYD Out-of-Network CYD + 50% CYD + 20% CYD + 40% Out-of-Pocket Maximum In-Network $2,000/$4,000 $3,500/$7,000 $5,800/$11,600 Out-of-Network $5,000/$10,000 $14,000/$28,000 $11,600/$23,200 $0 Combined with In-Network CYD Prescription Drug Program Rx Deductible Retail $10/$30/$50 100% after CYD BlueRx Discounts Only (Generic/Brand/Non-Preferred) Mail-Order $25/$75/$125 100% after CYD MONTHLY RATES CURRENT RENEWAL CURRENT RENEWAL CURRENT RENEWAL Employee Only $1,087.09 $1,239.84 $726.68 $828.80 $535.98 $611.31 Employee + Spouse $2,587.27 $2,950.82 $1,634.99 $1,864.73 $1,032.28 $1,177.34 Employee + Child(ren) $2,043.72 $2,330.90 $1,291.50 $1,472.98 $815.41 $930.00 Family $3,451.50 $3,936.49 $2,181.12 $2,487.61 $1,377.10 $1,570.61 MONTHLY EMPLOYER COST Total Monthly Premium (based on 22 enrolled) $23,915.98 $27,276.48 Monthly Increase $3,360.50 Annual Increase $40,326.00 Percentage of Increase 14.05% 1 CYD = Calendar Year Deductible 2 In-Network Advanced Imaging Services = MRI, MRA, PET, CT & Nuclear Medicine This matrix is only a highlight of the many benefits and services provided or authorized by Blue Cross and Blue Shield of Florida, Inc. and does not constitute a contract. Page 2
Citrus County Mosquito Control District 2020 Florida Blue Renewal Employer-Sponsored Alternate CURR RRENT CRO ROSSWALK BlueOptions BlueOptions Predictable Cost 5461 All Copay 14001 Deductible (per person/family) In-Network $250/$750 $250/$750 $1,000/$3,000 Out-of-Network $1,000/$3,000 Coinsurance (amount member pays) In-Network 10% 10% Out-of-Network 50% 50% $0 Wellness (Routine Exam, Well Woman Exam, Family Physician $0 Mammogram, Well Child) Specialist $0 $0 Coinsurance Coinsurance Out-of-Network Physician Office Services Family Physician $10 $10 $25 Specialist $25 CYD 1 + 50% Out-of-Network CYD + 50% $250 Inpatient Hospital Facility (per admission) Option 1 $250/day ($750 max) $375 Option 2 $375/day ($1,125 max) Out-of-Network CYD + 50% CYD + 50% $100 ER Facility (copay waived if admitted) In-Network $100 Out-of-Network $100 $100 Outpatient Hospital Facility Option 1 $100 $150 $150 Option 2 $200 Out-of-Network CYD + 50% CYD + 50% Provider Services at Hospital & ER $50 $0 $50 Independent Diagnostic Testing Facility In-Network $50 Advanced 2 $75 $75 CYD + 50% Out-of-Network CYD + 50% Independent Clinical Lab In-Network $0 $0 CYD + 50% Out-of-Network CYD + 50% Out-of-Pocket Maximum (includes CYD, $2,000/$4,000 In-Network $2,000/$4,000 Coinsurance, Copays, & Rx on ACA 3 ) Out-of-Network $5,000/$10,000 $5,000/$10,000 Prescription Drug Program Rx Deductible $0 $0 Retail $10 $0/$4/$10 Generic (Preventive/Condition Care/All Other) Brand (Condition Care/All Other) $30 $15/$30 $50/NA Non-Preferred/Speciality $50/$150 Mail-Order $25/$75/$125 2X Copay for 3 Months MONTHLY RATES Employee Only $1,239.84 $1,064.83 Employee + Spouse $2,950.82 $2,129.66 Employee + Child(ren) $2,330.90 $1,969.94 Family $3,936.49 $3,034.77 MONTHLY EMPLOYER COST Total Monthly Premium (based on 22 enrolled) $27,276.48 $23,426.26 Monthly Increase $3,360.50 -$489.72 Annual Increase $40,326.00 -$5,876.64 14.05% Percentage of Increase -2% Current Monthly Employee Only Rate $1,087.09 Current Monthly Premium $23,915.98 1 CYD = Calendar Year Deductible 2 In-Network Advanced Imaging Services = MRI, MRA, PET, CT & Nuclear Medicine 3 Prescription copays DO NOT count towards the Out-of-Pocket maximum on Plan 5461. This matrix is only a highlight of the many benefits and services provided or authorized by Blue Cross and Blue Shield of Florida, Inc. and does not constitute a contract. Page 3
Citrus County Mosquito Control District 2020 Florida Blue Renewal As-Is Renewal with Contributions PLAN N A PLAN N B PLAN N C BlueOptions BlueOptions BlueOptions Predictable Cost 5461 HSA-Compatible 5070/5071 HSA-Compatible 5022/5023 Deductible (per person/family) In-Network $250/$750 $3,500/$7,000 $2,500/$5,000 Out-of-Network $1,000/$3,000 $7,000/$14,000 $5,000/$10,000 Coinsurance (amount member pays) In-Network 10% 0% 20% Out-of-Network 50% 20% 40% Wellness (Routine Exam, Well Woman Exam, Family Physician $0 $0 $0 Mammogram, Well Child) Specialist $0 $0 $0 Out-of-Network Coinsurance Coinsurance Coinsurance Physician Office Services Family Physician $10 CYD CYD + 20% Specialist $25 CYD CYD + 20% CYD 1 + 50% Out-of-Network CYD + 20% CYD + 40% Inpatient Hospital Facility (per admission) Option 1 $250 CYD CYD + 20% Option 2 $375 CYD CYD + 20% Out-of-Network CYD + 50% CYD + 20% CYD + 40% ER Facility (waived if admitted) In-Network $100 CYD CYD + 20% Out-of-Network $100 CYD + 20% CYD + 40% Outpatient Hospital Facility Option 1 $100 CYD CYD + 20% Option 2 $150 CYD CYD + 20% Out-of-Network CYD + 50% CYD + 20% CYD + 40% Provider Services at Hospital & ER $50 CYD CYD + 20% Independent Diagnostic Testing Facility In-Network $50 CYD CYD + 20% Advanced 2 $75 CYD CYD + 20% Out-of-Network CYD + 50% CYD + 20% CYD + 40% Independent Clinical Lab In-Network $0 CYD CYD Out-of-Network CYD + 50% CYD + 20% CYD + 40% Out-of-Pocket Maximum In-Network $2,000/$4,000 $3,500/$7,000 $5,800/$11,600 Out-of-Network $5,000/$10,000 $14,000/$28,000 $11,600/$23,200 Prescription Drug Program Rx Deductible $0 Combined with In-Network CYD Retail $10/$30/$50 100% after CYD BlueRx Discounts Only (Generic/Brand/Non-Preferred) Mail-Order $25/$75/$125 100% after CYD MONTHLY RATES Employee Only $1,239.84 $828.80 $611.31 Employee + Spouse $2,950.82 $1,864.73 $1,177.34 Employee + Child(ren) $2,330.90 $1,472.98 $930.00 Family $3,936.49 $2,487.61 $1,570.61 EMPLOYEE CONTRIBUTION SUMMARY Monthly HSA Monthly HSA Payroll Deduction Payroll Deduction Payroll Deduction Contribution 3 Contribution 3 $0.00 Employee Only $0.00 $294.04 $0.00 $294.04 Employee + Spouse $1,710.98 $624.89 $0.00 $0.00 $62.50 $1,091.06 Employee + Child(ren) $233.14 $0.00 $0.00 $309.84 Family $2,696.65 $1,247.77 $0.00 $330.77 $0.00 1 CYD = Calendar Year Deductible 2 In-Network Advanced Imaging Services = MRI, MRA, PET, CT & Nuclear Medicine 3 Monthly HSA Contribution for Employee Only coverage has been calculated to avoid excess contributions. Page 4
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries