Economics at the Bedside: A bridge too far? Rakesh Patel M.D. Pharm.D. M.Sc September 29 th , 2016
Regret, Religion and Rationing: A bridge too far? “In my job as a physician, I have been troubled, at times, by my role in the lives that we extend through our interventions” Letter to the Editor Ottawa Citizen March 2008 S. Kravcik M.D. Div. General Internal Medicine, TOH Edvard Munch “ The Scream ” 1893-94
Regret, Religion and Rationing: A bridge too far? The nature of suffering and the goals of medicine. Cassel EJ NEJM 1982;306:639-45 “the relief of suffering and the cure of disease must be seen as the twin obligations of a medical profession that is truly dedicated to the care of the sick” “Physicians” [ and families ] failure to understand the nature of suffering…….. Becomes a source of suffering itself
Economics at the bedside: A bridge too far? “Do not try to live forever, You will not succeed” 1906
Economics at the bedside: A bridge too far? “ the art of medicine is to humour the patient while nature does the healing ”
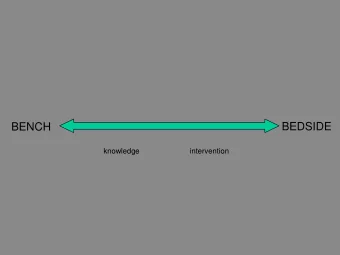
Economics at the bedside: A bridge too far? Dilemmas to ponder: The most expensive care is not the best care. .. . . Man-made & influenced healing what can we afford?
Economics at the bedside: A bridge too far? Cases to ponder: 1. Meet Pietro: 21yo who overdoses, ends up in ICU. He desperately needs psychiatric help His family: feels helpless, hopeless and dismissed How do we break his cycle of ED / ICU visits? What should we consider / do?
Economics at the bedsider: A bridge too far? Psychiatry ward?
Economics at the bedside: A bridge too far? Cases to ponder: 2a. Meet Letisha: Based upon your history taking, physical examination and Chest X-ray review, you diagnose her with Pneumonia She and her family want a C.T scan Your Attending wants a differential of what else may be causing her breathing problem
Economics at the bedside: A bridge too far? Cases to ponder: 2b. Meet Letisha: You order a C.T. The family adores you because you are an attentive & thoughtful, comprehensive doctor “ they felt they were in your care ! ” Your Attending rewards you for thinking broadly & ordering more tests to assess your hypotheses. You inadvertently drive up the cost of Pneumonia management!
Economics at the bedside: A bridge too far? Cases to ponder: 2c. Meet Letisha: And so it begins for doctors – the wrong incentives framework subliminally placed during training Lifelong lesson Patient-centred care, right?
Economics at the bedside: A bridge too far? Cases to ponder: 3a. Meet Jasna: You are the head of the P&T committee at your hospital. A 57yo who has a rare disorder with very few effective treatment(s) for control, none for cure She desperately needs treatment or she will die The cost of tx = $10K per cycle [n=5 cycles] She & her family feel helpless & hopeless
Economics at the bedside: A bridge too far? Cases to ponder: 3b. Meet Jasna: The treatment team presses you to approve the costly tx’s The hospital cannot afford multiple cycles The MoH refuses to pay for tx – lack of evidence What would you consider / do?
Economics at the bedside: A bridge too far? Cases to ponder: 4. Meet Vishnu Vishnu is now seen for the 3 rd time in a month with hyperglycemia despite being prescribed 2 different medications and being taught how to check his sugar daily You ask him, “ are you taking your insulin ?” He answers, “yes” Wrong question! Patient-centred care, right?
Economics at the bedside: A bridge too far? Cases to ponder: 5. Meet Penelope Penny has a wicked family hx of HTN & its complications Penny was wilfully non-compliant with her HTN tx Penny is now in the ICU with a large stroke Penny has cost our health-care system a lot of money Not enough personal / family responsibility for healthcare. What should we do here?
Economics at the bedside: A bridge too far? Cases to ponder; 6. Trying to get folks home Limited community palliative care resources Limited home-care resources Forces patients and families to seek out acute care hospital resources
Economics at the bedsider: A bridge too far? Universal Case; My __________ is a fighter(!), doctor. I forbide you to give up! We don’t want to believe that the patient has given up - that is unthinkable of our hero(s)
Economics at the bedside: A bridge too far? 1. Cost-effectiveness The degree to which something is effective or productive in relation to its cost. 2. Opportunity cost A $ spent here cannot be spent there
Economics at the bedside: A bridge too far? Is there a place for the principles of; 1. Cost-effectiveness 2. Opportunity cost In medical education and at the bedside?
Economics at the bedside: A bridge too far? “the ethics of the Hippocratic physician makes yes or no decisions on the basis of the benefit of a single patient without taking into account what economists call, “alternative costs” R.Veatch 1991 Will this thinking destroy; 1. The patient-physician relationship 2. A publicly-funded health care system?
Economics at the bedside: A bridge too far? 1. Cost-effectiveness 2. Opportunity cost Can a Clinician remain a patient advocate while serving as a steward of limited health-care resources? Can we define / teach ethical Clinician advocacy? See example of Letisha
Economics at the bedside: A bridge too far? 1. Cost-effectiveness 2. Opportunity cost How should we go about equitably distributing finite resources? See example of Pietro
Economics at the bedside: A bridge too far? 1. Cost-effectiveness 2. Opportunity cost How should we help clinicians appreciate that their decisions translate into expenses for their patients? See example of Vishnu
Regret, Religion and Rationing: A bridge too far? The Canada Health Act: Public Administration Comprehensiveness Universality Portability Accessibility
Clash of cultures, values & priorities? Changing demographics [“ silver tsunami ” ] Life-extending therapies Patient-centred care Greater & unrealistic expectations of the health-care system Are we making publicly-funded health-care unsustainable?
I now have cancer, where is my cure?
Economics at the bedsider: A bridge too far? I am entitled to my entitlements! I’ve paid my taxes! I want everything done!
Economics at the bedside: A bridge too far? MEDICAL ASSISTANCE IN DYING: A PATIENT-CENTRED APPROACH Report of the Special Joint Committee on Physician-Assisted Dying Hon. Kelvin Kenneth Ogilvie and Robert Oliphant Joint Chairs FEBRUARY 2016 42 nd PARLIAMENT, 1 st SESSION
Regret, Religion and Rationing: A bridge too far? Pneumonia may well be called the friend of the aged. Taken off by it in an acute, short, not often painful illness, the old man escapes those cold gradations of decay, so distressing to himself and to his friends W. Osler
Economics at the bedside: A bridge too far? 100% Life is a sexually transmitted fatal disease QOL & IADLs Time
Regret, Religion and Rationing: A bridge too far? ICU team – Family communications: Existence versus Life I want life in my years….. not years of life….
Regret, Religion and Rationing: A bridge too far? Major Principles of Health Care Ethics: Respect for Individual autonomy Beneficence: do good Nonmaleficence: don’t hurt Distributive justice: equal access and save some for the next guy [Egalitarian?]
Economics at the bedsider: A bridge too far? Rationing [ yes ] vs Waste avoidance [ yes ]? Ethical imperative; Unlimited demand Limited resources Fairest means of allocating such resources equitably? Accommodation of Distributive justice & Patient autonomy
Regret, Religion and Rationing: A bridge too far? 18 th Century Philosophers 20th Century Autonomy of Autonomy Individual city states of people Patient Autonomy A bridge too far ?
Regret, Religion and Rationing: A bridge too far? “ an injustice anywhere, is a threat to justice everywhere !” M.L. King Distributive justice
Economics at the bedsider: A bridge too far? Beach MC et al
Economics at the bedsider: A bridge too far?
Economics at the bedsider: A bridge too far? 83% response rate, n=414/500
Economics at the bedsider: A bridge too far? Rationing vs Waste avoidance? So… … …. . .Waste Eliminate waste : one-time savings approach only? [demand?] Stop spending on non-beneficial interventions [I want an MRI!]
Economics at the bedsider: A bridge too far?
Economics at the bedsider: A bridge too far? So… … What drives Cost ? Virtually unbounded patient demand and expectations Technological advances: tests, meds, devices, procedures Intervention drift / creep
The life cycle of any Drug Panacea! Poison! Pedestrian Bernard McDonald M.D. Ottawa Heart Institute
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries