District- -based risk based risk- -need need- -driven Personalized Care Program (PCP) for severe driven Personalized Care Program (PCP) for severe District District-based risk-need-driven Personalized Care Program (PCP) for severe mentally ill (SMI) using case management approach- -why, how, effective? why, how, effective? mentally ill (SMI) using case management approach mentally ill (SMI) using case management approach-why, how, effective? Dr. W K LEE, Consultant Psychiatrist, Kwai Chung Hospital, Hong Kong, China
Lecture outline Lecture o Enter your title here Lecture outline 1.Why? 2.How? 3.Effective? Kwai Tsing Tsing Personalized Care Personalized Care Programme Programme Kwai Page 2
Unmet service need About 22% of the global burden of DALYs has been attributed to mental disorders, mostly due to the chronically disabling nature of depression, schizophrenia and bipolar disorders and other mental disorders (1). The World Health Report 2001 on Mental Health “New Understanding, New Hope” has recommended that community care has a better effect than institutional treatment on the outcome and quality of life of individuals with chronic mental diseases (2). Shifting patients from mental hospitals to care in the community is also cost effective and respects human rights. Mental health services should therefore be provided in the community. However, there was also concern that under-funding in the deinstitutionalization process without safe quality community care support had produced an influx of the homeless, unemployed, offenders with increased risk of violence to themselves and public, and suicide particularly in people suffering from SMI or co-morbidity (3). There were also reports of increases in medical noncompliance and hospital readmission (4). As a reaction to some of these less desirable ramifications of deinstitutionalization, various models of community care were developed. 1. Prince M, Patel V, Saxena S et al. No health without mental health. Lancet 2007; 370; 9590: 859 – 877 2. The World Health Report on Mental Health “New Understanding, New Hope” 2001 3. Lamb HR, Weinberger LE. The shift of psychiatric inpatient care from hospitals to jails and prisons. J Am Acad Psychiatry Law. 2005; 33(4)529-534 4. Montgomery & Kirkpatrick. Understanding those who seek frequent psychiatric hospitalizations. Arch Psychiatr Nurs. 2002; 16 (1):16-24 Kwai Tsing Tsing Personalized Care Personalized Care Programme Programme Kwai
Why a new need-risk-driven, value-based, quality-focused, outcome-guided, recovery-orientated, district-based personalized care model for SMI patients in Hong Kong? 1. Clinical reasons Risk reduction: violence to others and suicide Enhance outcome towards recovery not only maintenance: advances in pharmacology and in cognitive therapies allow many patients to be treated successfully and to recover full health or to maintain their lives successfully with good functioning, social inclusion and quality of life, which is best predicted by level of unmet needs. Ensure good service compliance for better outcome and avoiding wastage of our resources 2. Value-based reasons Shared care: modern concepts of self-management and person-centered care mean that it is no longer acceptable to treat patients as passive recipients of services Support to families and carers 3. Socio-economic reasons Reduction of burden of illness and lost productivity 4. Service system and cost-effectiveness reasons Huge caseload unable to be managed by traditional CPS service model More cost-effective management by district-based general adult team with CMHT model Kwai Tsing Tsing Personalized Care Personalized Care Programme Programme Kwai
Why using case management model? International evidence Systematic reviews and meta-analyses showed the evidence for effectiveness of case management models as follows (1-5) 1. Healthcare service utilization: reduced number of hospital days, cost of hospital care and hospital admission, especially among patients who are high service users; 2. Clinical-psycho-social domains: improved clinical symptomatology, quality of life, housing stability, independent living, social functioning, employment, engagement and compliance with services, family and patient satisfaction; reduced family burden. 1. Mueser KT, Bond QR, Drake RE et al. Models of Community Care for Severe Mental Illness: A Review of Research on Case Management Schizophrenia Bulletin, 1998; 24(l):37-74 2. Ziguras SJ, Stuart GW. A Meta-Analysis of the Effectiveness of Mental Health Case Management Over 20 Years. Psychiatr Serv 2000; 51:1410-1421 3. Marshall M, Lockwood A. Assertive community treatment for people with severe mental disorders. Cochrane Database of Systematic Reviews 1998, Issue2 4. Smith L, Newton R. Systematic review of case management. Australian and New Zealand Journal of Psychiatry 2007; 41:2-9 5. Marshall M et al. Assertive community treatment – is it the future of community care in the UK. International Review of Psychiatry , 2000, Vol 12 (3) 191-196 Kwai Tsing Tsing Personalized Care Personalized Care Programme Programme Kwai
Why using case management model? Local evidence A 2-year randomized controlled trial conducted in KCH supported by research fund has proven that the case management model is a cost- effective way to discharge long stay schizophrenic patients and keep them in community with no undue readmission or deterioration in mental state. It showed better discharge rates; lower length of stay (LOS), higher adherences to community treatment programs, and better outcome measures on mental state as well as on quality of life. The increased discharge rate did not generate untoward social consequences, like delinquency or violence (1). A similar study in CPH with case management model of care on 20 chronic schizophrenic patients also demonstrated a significant reduction of LOS and number of readmissions (2). 1. Lee CC, Chiu SN, Wong CW, Ku B et al. The second deinstitutionalization project for severely mentally ill patients in Kwai Chung Hospital: a randomized controlled trial. Hong Kong Med J 2008; 14(Suppl 3):S36-40 2. Yuen MK et al. Application of case management in CPNS: Sharing session on case management in HAHO, February 2002 Kwai Tsing Tsing Personalized Care Personalized Care Programme Programme Kwai
Why district- -based risk based risk- -need need- -driven case management driven case management Why district approach for severe mentally ill (SMI)? approach for severe mentally ill (SMI)? 1. Well integrated district-based community mental health team (CMHT) that jointly manage and co-locate key elements of local acute mental health services, achieve the most positive outcomes for patients in terms of: (1) Preventing avoidable admissions Fewer delayed discharges and shorter duration of stay Improved understanding and flexibility of staff skills Better informed and coordinated care planning and risk management Improved cost-effectiveness 2. addresses district population-specific service needs; allows greater capability to respond to sudden and irregular crises; provides deeper coverage of services for community SMI patients by case managers possessing generic core competencies and discipline-specific expertise; who include a flexible staff mix of psychiatric nurses, occupational therapists, social workers; improves efficiency and cost-effectiveness of service delivery. 1. Laying the Foundations for Better Acute Care. Department of Health Estates and Facilities Division, UK. 2008 Kwai Tsing Tsing Personalized Care Personalized Care Programme Programme Kwai
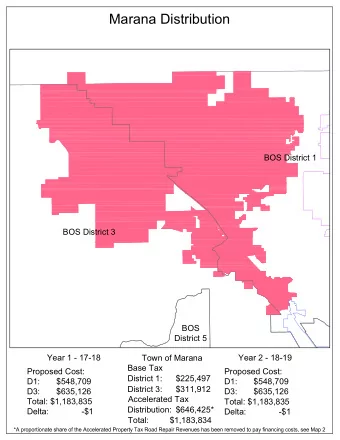
Enter your title here PCP Target Deliverables (Pilot in 2010/2011) PCP PCP Target Deliverables (Pilot in 2010/2011) YUEN LONG YUEN LONG 3,415/ 1515 3,415/ 1515 KWAI TSING KWAI TSING 4,033/ 1515 4,033/ 1515 KWUN TONG KWUN TONG 4,253/1560 4,253/1560 Pilot district Pilot district SMI Population / Target Headcount SMI Population / Target Headcount Page 8 Kwai Tsing Tsing Personalized Care Personalized Care Programme Programme Kwai Page 8
Enter your title here PCP Programme Objectives PCP PCP Programme Objectives 1. To develop a community-based personalized (patient-centered) care programme using a case management model 2. To provide coordinated care based on needs and risk assessment (needs and risk management) 3. To prevent avoidable hospitalization by better engagement (gate- keeping) 4. To reduce disabilities and enhance recovery by promoting social inclusion (recovery-focused care) 5. To establish a district-based platform for better service coordination (community partnership) 6. To build up professional workforce to meet future service reform (workforce development) Page 9 Kwai Tsing Tsing Personalized Care Personalized Care Programme Programme Kwai Page 9
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries