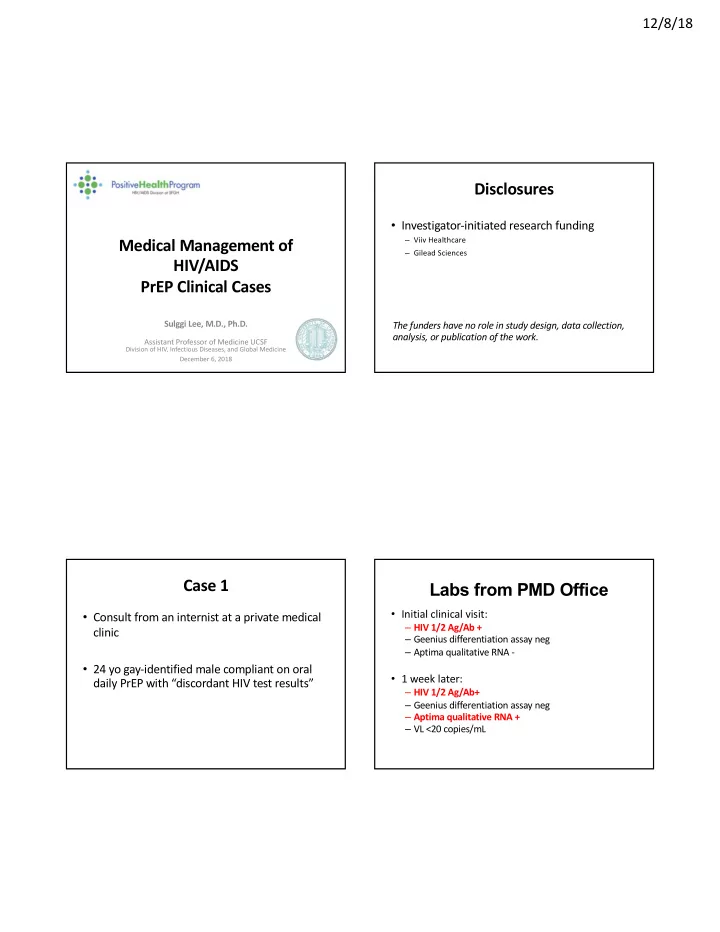
12/8/18 Disclosures • Investigator-initiated research funding Medical Management of – Viiv Healthcare – Gilead Sciences HIV/AIDS PrEP Clinical Cases Sulggi Lee, M.D., Ph.D. The funders have no role in study design, data collection, analysis, or publication of the work. Assistant Professor of Medicine UCSF Division of HIV, Infectious Diseases, and Global Medicine December 6, 2018 Case 1 Labs from PMD Office • Initial clinical visit: • Consult from an internist at a private medical – HIV 1/2 Ag/Ab + clinic – Geenius differentiation assay neg – Aptima qualitative RNA - • 24 yo gay-identified male compliant on oral • 1 week later: daily PrEP with “discordant HIV test results” – HIV 1/2 Ag/Ab+ – Geenius differentiation assay neg – Aptima qualitative RNA + – VL <20 copies/mL
12/8/18 Case Timeline Plasma RNA HIV Measurements CLINICAL VISIT : STD TESTING - HIV 1/2 Ag/Ab POS - Cell-associated DNA - Geenius differentiation neg - Aptima “qualitative” RNA neg - Cell-associated RNA - Plasma HIV RNA CLINICAL VISIT 2: STD TESTING - HIV 1/2 Ag/Ab POS - Geenius differentiation neg - Aptima “qualitative” RNA POS - HIV RNA <20 Exposure PrEP x 1 year RESEARCH STUDY BASELINE - HIV 1/2 Ag/Ab neg - Plasma HIV RNA <40 - Detuned 0.07 (neg or acute) RESEARCH ASSAYS - Ultrasensitive Plasma HIV RNA neg - Cell-associated DNA neg - Cell-associated RNA POS 2/2 reps = 117 copies/10 6 PBMCs Repeat testing neg -12 mo - 3 mo -1 mo -2 wk 0 1 wk 1 mo 2 mo x 1 2 g e P e # # 1 s # E n g g r y P V c n n t i i s i I n t t d H s s v i e e ) e ) e ) u P P g t t P t t y r s q E E d u a a E e ) c c r P i r i r u d t L r r n P n P t S P f E i i S - ( l n l n 4 h r C C g P o o d H i n ( ( e o t r ( a Time t ) S T Pasternak Retrovirology 2013 R ( A Clinical Plasma HIV RNA Assays Can PrEP be “Overwhelmed?” • Aptima TMA – false positive = 0.5% • Unpublished data modeling from Bob Grant’s SeroPrEP study – (1 out of 200) were falsely positive when truly negative (compared to a cell-associated DNA). – Suggests that >90 sex acts per month might be a – Only a 0.5% chance that this is a false positive. “threshold” that could surpass daily oral PrEP • Case report of 1 man who has sex with men who was infected with wildtype virus while highly adherent to daily TDF/emtricitabine Hoornenborg CROI Feb 2017, Seattle WA #953 Fiscus JCM 2013; Pas JCM 2013
12/8/18 Effects of PrEP on NAT and Antibodies Incidence Assay Performance in Early HIV Infection Acute HIV Infection Reduces and delays • RNA and p24 RNA/p24 Ag – Can be below LOD of IgM antibodies NAT IgG antibodies • Reduces and delays IgM and IgG responses But what does PrEP do to the timing of positivity and – Can get false neg on “4 th Gen” EIAs interpretation of these tests?? Acute HIV Infection on PrEP • Can get seroreversion • Bands on western Antiretroviral therapy blot/anti-HIV RNA/p24 Ag antibody tests may be delayed and atypical IgM antibodies IgG antibodies Keating CID 2016 National HIV Curriculum at https://www.hiv.uw.edu/go/screening-diagnosis/diagnostic-testing/ Antibody Response is “Aborted” with Early ART PrEP Interference with Incidence Testing and Resumes with Treatment Interruption • Suppressed viral replication – False neg even with the most sensitive NAT assays N = 7 aviremic N = 10 viremic • Interference with serological response in patient – False neg antibody results, delayed responses, seroreversions with EIA and WB (Hare CID 2006; Killian AIDS Res Hum Retr 2006; Stephenson OFID 2016) • Unusual patterns of serology and NAT testing – NAT ‘positive’ signal without seroconversion – Negative, indeterminate western blots/EIAs Stephenson OFID 2016
12/8/18 PrEP Demo Participant Started ART Implications for HIV Cure ~12 Days after HIV Infection . . . Virus Persists in Dormant T Cells Patient started on ART ~10 days from infection 220 copies/mL ART DO NOT kill these cells! Henrich Deeks PLoS Med 2017 Stevenson Scientific American 2008 Decided to Undergo Analytic Treatment Case Summary Interruption – Rebounded at Day 230 • Very difficult to definitively confirm if patient was Day 230 indeed HIV+ CD4+ Count – Patient elected to continue with full ART – No issues with stigma or carrying diagnosis of HIV – PMD in agreement given high risk sex activity • Alternatives – Remain on PrEP and monitor Plasma HIV RNA • If new HIV infection – will not know if new or early suppressed? – Analytic treatment interruption off all therapy • Not feasible given high risk frequent sex • Unclear length of follow-up to assess viral rebound Henrich Deeks Plos Med 2017
12/8/18 - STAT PAK neg - STAT PAK neg - STAT PAK neg - STAT PAK neg Case 2 - Pooled RNA neg - Pooled RNA neg - Pooled RNA neg - Pooled RNA neg - Urine GC pos - Urine GC pos - 4 Partners - 3 Partners - Urine GC pos - 2 Partners - 3 Partners - Genital HSV-2 PCR pos - STAT PAK neg - 4 Partners - Pooled RNA POS (529 copies/mL) - Urine GC POS - 5 Partners • 21 year-old Latino man who has sex with male, - Ag/Ab POS cis female and trans female partners, on oral daily - Geenius POS - HIV RNA 1,544 copies/mL Testing PrEP • Reported “excellent adherence” • At 13-month PrEP visit, rapid HIV Ab neg 0 3 6 10 12 13 13.3 14 • But 5 days later, plasma HIV RNA = 559 copies/mL n o T i a t R i A t i n g I u P r Months E D r - P 4 adapted from Cohen Lancet HIV 2018 - STAT PAK neg - STAT PAK neg - STAT PAK neg - STAT PAK neg Case Continued - Pooled RNA neg - Pooled RNA neg - Pooled RNA neg - Pooled RNA neg - Urine GC pos - Urine GC pos - 4 Partners - 3 Partners - Urine GC pos - 2 Partners - 3 Partners - Genital HSV-2 PCR pos - STAT PAK neg - 4 Partners - Pooled RNA POS (529 copies/mL) - Urine GC POS - 5 Partners • To evaluate for possible early suppressed - Ag/Ab POS - Geenius POS infection - HIV RNA 1,544 copies/mL Testing – Additional testing of stored plasma from the visit Geno/Pheno - RT: L74V, L100I, High adherence by hair M184V, K103N 12 weeks prior to the diagnosis visit - FTC resistant but TDF susceptible (no K65R) • No evidence of plasma HIV by iSCA (lower limit of detection = 1 copy per /ml) High adherence by DBS – Single Genome Sequencing on early sample • Limited viral diversity consistent with acute infection 0 3 6 10 12 13 13.3 14 n o T i a t R i A t i n g I u P r Months E D r - P 4 adapted from Cohen Lancet HIV 2018
12/8/18 PrEP Failure is RARE! Worldwide Reported PrEP Failures • There are only a few cases reported worldwide 5 cases emtricitabine/tenofivir failure All compliant with PrEP – Hundreds of thousands of people have used PrEP – Tens of thousands of HIV infections have been 4 multiresistant HIV prevented. 4 had M184V leading to high level resistance to FTC 2 viruses that were susceptible to TDF – Almost all people who use PrEP stay free of HIV Aberrancies in test results Low viral loads Delayed seroconversion The message to send your patients is that PrEP Indeterminate western blots is highly highly effective Cohen Lancet HIV 2018 Acknowledgements Case 2: Stephanie Cohen, Darpun Sachdev, Oliver Bacon, Mary Kearney, Susa Coffey, Bob Grant, Diane Havlir, Monica Gandhi Case 1&2: SCOPE TEAM Jeff Martin Rick Hecht Tim Henrich Kara Marson Top: Enrique Martinez-Ortiz, Viva Tai, Chris Pilcher, Mike Busch, Steven Deeks, Peter Hunt. Bottom: Monika Deswal, Montha Pao, Maya Ball-Burack, Rebecca Hoh, Heather Hartig, Marian Kerbleski, Sulggi Lee. Not pictured: Raeni Miller, Claire Lisa Harms Tony Ling Rappaport, Melissa Krone, Mary Ellen Kelly, Elnaz Eilkhani
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries