See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/11956283 Delayed Presentation of Compartment Syndrome following Gastrocnemius Tear Article in Acta orthopaedica Belgica · May 2001 Source: PubMed CITATIONS READS 7 943 3 authors , including: Matt D A Fletcher University of British Columbia - Vancouver 44 PUBLICATIONS 139 CITATIONS SEE PROFILE Some of the authors of this publication are also working on these related projects: Hip arthroplasty View project External fixation View project All content following this page was uploaded by Matt D A Fletcher on 04 June 2014. The user has requested enhancement of the downloaded file.
CASE REPORT DELAYED PRESENTATION OF COMPARTMENT SYNDROME FOLLOWING GASTROCNEMIUS TEAR M. D. A. FLETCHER, D. SPICER, P. J. WARREN The authors describe a case of acute compartment activities, and noted only persisting minor discom- syndrome occurring twenty days following a tear of fort. Twenty days following the initial episode, he gastrocnemius. To their knowledge, this is the only awoke with severe pain in the same leg and pre- such case reported where the onset of compartment sented to the Accident and Emergency department syndrome was so long since the index injury. immediately. Keywords : compartment syndrome ; gastrocnemius Examination revealed a grossly swollen and tear ; delayed presentation. tense right calf, which was tender to the touch over Mots-clés : syndrome de loge ; rupture du jumeau ; the anterior, lateral and posterior aspects, and apparition tardive. acutely painful on passive ankle dorsiflexion. ——————————————————————————— Peripheral pulses were present, but he was noted to have paraesthesiae over the lateral aspect of his foot in the distribution of the sural nerve, and INTRODUCTION objective loss of power in ankle dorsiflexion and plantarflexion. Acute compartment syndrome is a well recog- Ultrasound of the leg revealed a haematoma of nized complication of lower limb trauma. It has the superficial posterior compartment (fig. 1). A been recognized following partial tears of the gas- clinical diagnosis of compartment syndrome was trocnemius. Presentation usually occurs within 24 made, and while waiting for operative fasciotomy hours of such an injury. No case has yet been he was noted to have an increasing sensory deficit, described of a compartment syndrome occurring with loss of sensation over the dorsal and lateral weeks following a gastrocnemius tear. We describe aspects of the foot, and an ascending pattern of loss such a case presenting 20 days after a partial tear of over the anterolateral leg. the medial head of gastrocnemius. At surgery, a single longitudinal lateral incision was made, and a four compartment perifibular CASE REPORT fasciotomy was performed without resecting the fibula (3). The anterior and peroneal compartments A 51-year-old engineer presented to the were tense, and were released throughout their Accident and Emergency department with a sudden onset of pain in his right calf. Three weeks previ- ously he had been walking across a road, when he felt a sudden sharp pain, “like being shot” in the ———————— Department of Orthopaedic Surgery, Northwick Park same calf. He was able to continue walking, the Hospital, Harrow, Middlesex, United Kingdom. pain had subsided to an ache shortly after, and the Correspondence and reprints : M. D. A. Fletcher, 1 Long calf became only transiently swollen. During the Barnaby, Midsomer Norton, Bath BA3 2TZ, U.K. E-mail : following three weeks, he continued his usual matt.fletcher@doctors.org.uk. Acta Orthopædica Belgica, Vol. 67 - 2 - 2001
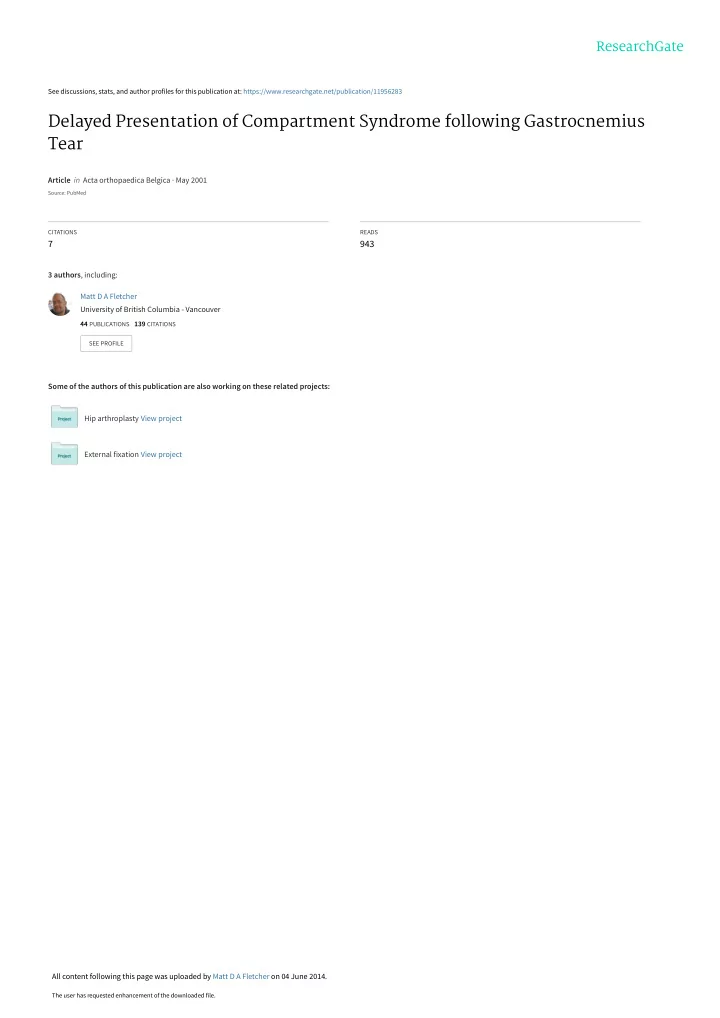
191 DELAYED PRESENTATION OF COMPARTMENT SYNDROME ment by osmosis, and increases the intrinsic com- partment pressure. Once this reaches a critical level, venous return is obstructed, and pressure rises steeply, with concomitant muscle ischaemia, oedema and necrosis. Increase of single compart- ment pressures can cause concomitant pressure rises in neighbouring compartments (4, 7). This would account for the findings in this case, and explain the involvement of the superficial and deep peroneal nerves. Liquefaction of a haematoma may lead to a delayed response, as in this case. Partial tear of the medial head of the gastrocne- mius is a common injury, due to overstretching of the muscle during ankle dorsiflexion (4). It occurs Fig. 1. — Ultrasound examination of both lower legs. The scan more commonly in middle-aged individuals, due to on the left shows the normal echodense appearance of gastroc- nemius and soleus. The scan on the right shows a hypoe- degenerative changes in muscle, and is not restrict- chogenic region consistent with a large haematoma in the ed to athletes (8). The injury is usually mild, and superficial posterior compartment. complications are rare (1). Acute compartment syn- drome is a rare complication (7). length, revealing grossly oedematous musculature. One case has been described where onset of the The fascia of the superficial posterior compartment compartment syndrome was delayed over a period was incised, digital examination revealed an old of 48 hours (2). Our case shows that a compartment haematoma and a palpable tear at the medial gas- syndrome may occur with a longer interval trocnemius myotendinous junction. The muscula- between the index injury and onset. Search of the ture of the deep posterior compartment was simi- literature has revealed no other case of an acute larly decompressed. The wound was dressed, and compartment syndrome presenting three weeks fol- left open. lowing lower limb trauma. Prompt recognition and Post-operatively he reported immediate relief of early fasciotomy led to complete recovery in this pain and regained complete sensation to the lower case. It is well documented that delay in treatment limb, with good motor power within 12 hours. The of compartment syndromes is associated with a wound was re-inspected at 48 hours and the mus- high amount of subsequent morbidity and disabili- culature of all compartments was deemed viable. ty (9). Compartmental pressure monitoring may be The wound was formally closed 5 days after pre- helpful in assessment of the patient with unclear sentation. The patient subsequently made a full pathology, and to document objective findings, but recovery, with no neurovascular deficit. surgical intervention should be largely based on clinical grounds (6). Pressure monitoring was not DISCUSSION performed in this case due to lack of available resources, and therefore all four compartments Acute compartment syndromes are most com- were decompressed due to the clinical findings of monly associated with severe muscle trauma and progressive nerve involvement. closed fractures of long bones. Less common asso- We hope by presenting this case to iterate that ciations include tight casts and non-traumatic soft- compartment syndromes may present following tissue injuries ; such as exertional damage and minor trauma, and that rarely, this may be weeks minor sporting injuries (5). The mechanisms following the index injury. A careful history will involved are those of bleeding into muscular com- alert the clinician to the possibility of a compart- partments, oedema and tissue necrosis. When ment syndrome despite no immediately preceding haematoma is present, water enters the compart- trauma. Acta Orthopædica Belgica, Vol. 67 - 2 - 2001
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries