
Council of governors general meeting 22 March 2017 Strategic update - PowerPoint PPT Presentation
Council of governors general meeting 22 March 2017 Strategic update David Evans, Chief executive Any questions? Recent IT issues network failure at North Tyneside General Hospital Mark Thomas, Director of health informatics Failure
Council of governors’ general meeting – 22 March 2017
Strategic update David Evans, Chief executive
Any questions?
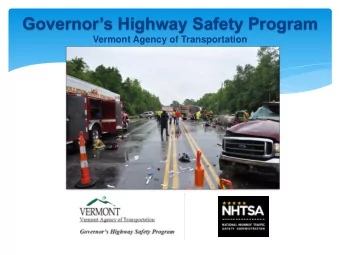
Recent IT issues – network failure at North Tyneside General Hospital Mark Thomas, Director of health informatics
Failure of core network
Any questions?
Annual plan and quality account Birju Bartoli, Executive director of performance and governance
Setting the scene Vision: To be the leader in providing high quality, caring and safe health and care services • Every year we produce a quality account to demonstrate how well we are performing as a trust on measures of quality including; patient safety, clinical effectiveness and patient experience • Continuing to improve quality is our absolute priority and this means making sure our patients get the best possible outcome and experience every time they need our care
Annual planning process • Five year strategic plan (2014 – 2019) – overall direction, what we are about • Changed to two year planning cycle - plan for 2017/18 to 2018/19 • Safety and quality objectives for 2017/18 • Quality strategy • Quality account covering 2016/17 – statutory requirement to inform public of delivery of safety and quality priorities • Annual report and corporate governance statement • Engagement with key stakeholders
Safety and quality objectives – 2017/18 • Five key areas agreed at the trust’s clinical policy group • Linked explicitly to the trust’s quality strategy • Objectives supported by governors and stakeholders • Some objectives building on 2016/17 objectives and embedding changes • Use of clear language when describing trust’s objectives
Safety and quality objectives 2017/18 • Five key areas: o To drive improvements in the quality of care and services provided for patients suffering from breathlessness o To improve the quality of care and services for older people o To continue to improve the management of sepsis in hospital and community settings o To implement the flow project to reduce delays in the system o To improve the timeliness and quality of treatment for patients who visit us with abdominal pain
Quality account 2016/17 • Look back at safety and quality priorities for 2016/17 and those agreed for 2017/18 • Standard requirements for all trusts to report • Including information on mortality and preventable deaths, areas of achievement • Quality account for 2017/18 process underway - to be completed by end April 2016 – for stakeholder comment in May 2016 • NHS Improvement guidance on mandatory indicators – no change • Governor selected local indicator
Quality account 2016/17 • As per guidelines, two indicators required for limited assurance opinion by KPMG • Based on national annual reporting guidance • Acute trusts required to be audited against two indicators: - 18 weeks referral to treatment * - A&E four hour 95% target * • Patient experience to remain the governor selected local indicator to be externally audited
Our performance on our priorities 2016/17 Safer Care Performance On or Better than Target, Below Target, As Expected Reduce hospital acquired infections (Cdiff, MRSA, SSI) Improve management of sepsis in hospital and community settings Falls and pressure ulcers (based on safety thermometer) National safety standards for invasive procedures (Nat SSIPs) Medicine optimisation Electronic prescribing roll out Antimicrobial stewardship
Our performance on our priorities 2016/17 High Quality Care Performance On or Better than Target, Below Target, As Expected Elderly trauma pathway Discharge / flow Electronic track and trigger tool (revised project plan) Dementia care pathway Mortality case note reviews Learning disabilities – care bundle COPD bundle Maternity bundle of care
Our performance on our priorities 2016/17 Patient Experience Performance On or Better than Target, Below Target, As Expected Patient experience – including kindness and compassion measure Alcohol management NHS staff health and well being
Quality account • Draft account ready mid April 2017 • Circulated to stakeholders for formal opinion end April • Final, including stakeholder comments, submitted to NHS Improvement and Parliament end of May • Upload to NHS Choices by end June 2017 • Written in line with annual reporting guidance – key measures and phrases used that are auditable
Any questions?
Accountable care organisation (ACO) update Birju Bartoli, Executive director of performance and governance
ACO - recap • System and collective leadership • Blurring the commissioner : provider divide • Red line letter submitted November 2016 • Clinical strategy discussions November 2016 • Outline business case submitted in December 2016 • Feedback and all parties meeting January 2017 • Approval to move to full business case submission
ACO – February onwards Development of: • Full business case • Clinical model – ‘industrialise / scale up what we do’ • ACO contract (ten years) • Governance arrangements - partners • Financial model (three years to balance) • Risk model • Regulation of the ACO • ACO business unit • Transition period
Clinical strategy “Our difficulty lies not so much in developing new ideas as in escaping from the old ones” John Maynard Keynes
Northumberland: Population Characteristics GP practices by locality Northumberland has a registered population of approximately 323,000 people, split into four localities: Blyth Central North West Valley Population 86,000 92,000 65,000 80,000 (27%) (29%) (20%) (25%) Number of 10 9 12 14 GP practices • The Blyth Valley and Central localities are more urban and densely populated, with a slightly younger population (80% and 79% aged under 65, respectively) • The North and West localities are more rural and sparsely populated, with a slightly older population (73% and 74% aged under 65, respectively) Source: GP registered population as at 1/01/2017 (https://data.gov.uk/dataset/numbers_of_patients_registered_at_a_gp_practice)
Population segmentation (acute data only): key findings This analysis looks at patient stratification and spend profiles using pseudonymised, patient-level, acute SLAM data from Northumberland CCG for the period November 2015 to October 2016 * . The patients captured within the data (inpatient, outpatient and A&E) have been stratified based upon activity and spend profiles across the Trusts through which acute services are commissioned by Northumberland CCG. Our analysis of patient-level, acute SLAM data from Northumberland CCG for the period November 2015 to October 2016 has found that: • 68% of acute spend comes from Northumbria Healthcare NHS Trust, 29% from Newcastle Upon Tyne Hospitals NHS Trust and 3% from other providers • 24% of Northumberland’s patients drive 80% of acute spend; these patients tend to be aged over 65, with a high usage of both inpatient and outpatient acute services * The A&E data relates to the period October 2015 to September 2016 25
Population patient stratification (for acute data only) Tier ier 1 and 2 patie tients driv rive acut cute spen end for r Northumberla land CCG Percentage of acute Percentage of acute spend service users 11,725 people use £90.0m of Tier 1: High cost patients and service 50% T1 Northumberland CCG users 8% services 24,276 people use 30% T2 £54.0m of Tier 2: Rising cost patients and service users 16% Northumberland CCG services 41,407 people use £27.0m of T3 15% Tier 3: Low cost patients and service users 27% Northumberland CCG services 5% 74,057 people use Tier 4: Lowest cost patients and service users T4 £9.0m of 49% Northumberland CCG services Source: SUS data, November 2015 to October 2016 Note: Patients are identified by a pseudo-NHS number provided in the SUS data set. Records without this data are excluded from the stratification analysis, accounting for 0.5% of total spend. Patients are ranked by descending total patient spend and segmented into tiers using the acute spend bands shown above. 26
Recommend








More recommend
Explore More Topics
Stay informed with curated content and fresh updates.