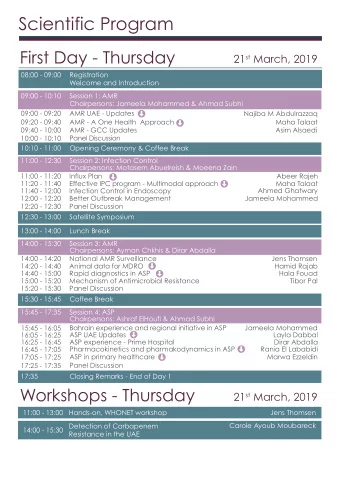
Central District Coordinating Council Quarterly Meeting October 22, 2019
Central District Coordinating Council (DCC) Infrastructure: State Coordinating Council for Public Health Update – Denise Delorie, SCC Representative Workgroup & Project Updates • Infectious Disease update – Donna Guppy, Field Epidemiologist • ACEs/Resiliency – Elizabeth Barron, Denise Delorie • District-wide Prevention Messaging – Nicole Poulin, Jim Wood • Partners for Recovery Grant – Brie Karstens • Vaccination Preparedness – Donna Guppy, Paula Thomson Maine Center for Disease Control and Prevention
Central District Coordinating Council (DCC) Infrastructure: Workgroup & Project Updates • ACEs/Resiliency – Elizabeth Barron, Denise Delorie • District-wide Prevention Messaging – Nicole Poulin, Jim Wood • Partners for Recovery Grant – Brie Karstens • Vaccination Preparedness – Donna Guppy, Paula Thomson Maine Center for Disease Control and Prevention
Central District Coordinating Council (DCC) Infrastructure: Prevention Services Contracts – any questions? • Substance Use Prevention • Tobacco Use & Exposure Prevention • Youth Engagement • ‘Let’s Go’ / Obesity Prevention Maine Center for Disease Control and Prevention
Central District Coordinating Council (DCC) A Youth Engagement and Empowerment Project: Youth Working on Their Own Anxieties in Order to Address Issues in their School April Hughes, Tobacco Prevention Coordinator Healthy Communities of the Capital Area Joanne Joy, Director Healthy Communities of the Capital Area Maine Center for Disease Control and Prevention
Central District Coordinating Council (DCC) Partners for Recovery Grant Stigma Assessment Results LeeAnna Lavoie, Director of Prevention Services MaineGeneral Prevention & Healthy Living Brianne Karstens, Community Programs Coordinator MaineGeneral Prevention & Healthy Living Maine Center for Disease Control and Prevention
Maine’s Central Public Health District Partners for Recovery Grant Stigma Assessment Preliminary Results October 22, 2019 Shane Gallagher, MS, CHES and Brie Karstens, BS
Partners for Recovery • The Partners for Recovery (PFR) project is working to reduce the impact of opioid use disorders (OUD) by: – Strengthening and expanding partnerships – Increasing treatment capacity – Implementing systems related to screening and referrals
Stigma Workgroup Central Public Health District Coordinating United Way of Council GRASP Mid Maine Healthy Health Reach Communities Community of the Capital Health Centers Area MaineGeneral Stigma Somerset Harm Reduction Public Health Workgroup Program
Assessing Stigma • Mixed method approach – Qualitative and quantitative – Surveys and focus groups – Assessed internalized, social and structural stigma • 3 different populations of interest – Individuals with lived Experience – Healthcare providers/front line staff – Community • Developed distribution plan
Methods Healthcare Individuals with Community Providers lived experience • Online • Focus groups • Online • Staff meetings • Online • WABI 5 • Doc notes • In person • Kennebec Journal/Morning • needle exchange Sentinel and • Community • Residential and Events treatment providers
Results 160 140 120 100 80 60 40 20 0 Front Line Staff Medical Staff Individuals w lived Experience Community
I personally know someone dealing with addiction Community N = 147 Nearly 90% of respondents know someone dealing with addiction
Addiction is a choice Community N = 147 Almost 80% of respondents said addiction is not a choice
Have you ever been discriminated against because of your current or past drug use? Individuals with lived experience N = 103 About 85% of respondents reported being discriminated against
My drug use has prevented me from getting the care that I needed. Individuals with lived experience N = 103 More than 50% of respondents reported their drug use prevented them from getting help
It is difficult and time consuming for me to manage MAT patients. Medical Provider N = 72 A little over 50% of respondents reported they don’t feel it’s difficult and time consuming to manage MAT patients
I routinely prescribe Narcan/Naloxone to all of my patients with OUD or their significant others Medical Provider N = 72
Addiction is a choice. Front About 65% of respondents said line staff addiction is not a choice N = 152 Of note 80% of community members reported addiction is not a choice
It’s okay to refer to someone as junkie, addict or abuser. Front Over 75% of respondents said it is line staff not ok to refer to someone as a N = 152 junkie, addict or abuser
Focus Group Results
Results Where have you experienced stigma? ▪ Trouble finding housing and Jobs background checks. “ I’m not the same person I was when I was using and for them to discriminate against me is screwed up. It’s over 10 years ago.” ▪ DHHS offices, family members, emergency department, Pharmacy, doctor’s office
Results How can people better support you staying in recovery? ▪ Help families understand what addiction and recovery is ▪ “My family asks are you tapering yet? When are you going to be done?” It’s super frustrating ▪ Understand how Suboxone/Methadone works ▪ Recognize success; “tell me I’m doing good”
Results Other barriers to recovery? ▪ Transportation ▪ Waitlists for programs ▪ Mental Health issues ▪ Having to come to so many appointments makes finding a job difficult ▪ Isolation – gentlemen referenced the Rat Park research.
Next Steps • USM to conduct a formal analysis • Develop strategies based on report to address stigma • Conduct assessment annually
QUESTIONS
Central District Coordinating Council (DCC) networking break… Statewide Community Naloxone Distribution and Ordering Process LeeAnna Lavoie, Director of Prevention Services MaineGeneral Prevention & Healthy Living Maine Center for Disease Control and Prevention
Community Naloxone Distribution District Coordinating Council Meeting October 22, 2019 MAINEGENERAL DRUG OVERDOSE PREVENTION AND HARM REDUCTION
What is the Community Naloxone Distribution Program? • State-funded program – Signed into effect by Governor Janet Mills on February 6, 2019 – 35,000 naloxone kits to be distributed in a one-year time frame • Intent: Widespread distribution of naloxone to high- risk patients throughout Maine
Naloxone Hubs
Public Health Distribution System Priorities • Note: Governor established priorities – High priority – non-profit, high need, low barrier service organizations – Lower priority – for-profit groups or groups with other sources of funding, like larger health care agencies CoAg Steering Committee 10/17/19
Tier 2 Profiles • T2 Partners can be one of • Some quick examples: any number of diverse – Portland Public Health organizations, some • Greater Portland Health examples include: • Preble Street • Cumberland County Jail – Harm Reduction Groups – MaineGeneral/MAP – Homeless Shelters • Western Maine Health – FQHCs • Bethel Health Center – County Jails • Knox County Jail – Schools – Bangor Public Health – Needle Exchanges • Health Equity Alliance • Downeast Treatment Center • Wabanaki Health and Wellness CoAg Steering Committee 10/17/19
Who is eligible for this program? • Intent: distribute naloxone for no cost to high-risk patients or loves ones who cannot otherwise access naloxone – Providers are encouraged to prescribe naloxone when possible • MaineCare patients are able to fill a prescription for naloxone every 28 days for little to no cost – Pharmacies are able to distribute with no prescription under their standing orders – High-risk patients/community members interacting with high-risk patients who cannot or will not fill a prescription are the ideal candidate
Logistics- How does this program work? 1. Orders are placed through SAHMS or through one of the distribution sites 2. Ordering organizations are assigned to a distributing agencies 3. Distribution agency will reach out to organization
Distribution Requirements • Signed MOU • Trained staff • Required monthly data tracking • Ongoing communication
How do you get involved? • Visit the SAMHS website to put in a request form https://www.maine.gov/dhhs/samhs/forms.shtml
How do you get involved? • Requests will be assigned to one of four distributing agencies o Portland Public Health o Bangor Public Health o MaineGeneral o Maine Access Point • The agency will reach out and schedule a training • After training, distribution can begin
Central Public Health Community Distribution • Received 30 orders • Trainings conducted: – Community-based organizations: 10 – Community Events: 20 – Next Step Needle Exchange: 15 • Kits distributed: – Community-based organizations: 698 – Events: 57 – NSNE: 15
Bangor Public Health Key: Prioritized/ In Active Process Maine General Agencies in Queue Tier 1 Hub Portland Public Health CoAg Steering Committee 10/17/19
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries