Cancer in low- and middle-income countries: what should we do? Franco Cavalli MD, FRCP Scientific Director Oncology Institute of Southern Switzerland CH-6500 Bellinzona
Cancer kills more globally! 8 7 6 Millions of victims 5 4 3 2 1 0 TB AIDS Malaria All 3 Cancer WHO (2003)
World Estimated Cancer Burden in 2030 Cases Deaths 2000 0 5 10 15 20 25 30 35 Millions 2030 (Population growth) 2030 (+1% annual increase of the risk) 2030 Annual percent change in Incidence (+1.3) and Mortality (-0.4) in France (1978-2000) Remontet et al., 2002
Cancer in developing countries 1970 15% of global burden 2008 56% of global burden 2030 ca. 70% of global burden
Global burden of cancers attributable to infections in 2008: a review and synthetic analysis (IARC) ! 2008 = 12.7 Mio. new cancer cases ! attributable fraction for infectious agents: 16.1% (2 Mio. cases) less developed countries 22.9% more developed countries 7.4% Variation: New Zealand 3.3% ! sub-Saharian Africa 32.7% H.Pylori, hepatitis B/C and HPV account 1.9 Mio. cases (95%) C. de Martel et al. Lancet Oncology 2012; 13:607-615
Cancer mortality (fatality ratio) 75% low income countries 72% middle income countries 64% upper-middle income countries 46% high income countries P. Farmer et al. Lancet 2010; 376:1186-93
Breast and cervical cancer in 187 countries between 1980 and 2010: a systematic analysis Breast cancer Cervical Cancer (thousands) (thousands) 1980 2010 1980 2010 cases 641 1600 378 460 deaths 425 (50-50%) * 220 (80-20%)* deaths < 49 yrs in 68 (70-30%) * 60 (85-15%) * developing countries ( ) * = proportion developing / developed countries 3.1% / year " incidence: 1980-2010 BC 0.6% / year " CC MH Forouzanfar et al. Lancet 2011; 378:1461-84
Breast Cervical Life GNI per head Health cancer cancer expectancy (2009 US$) expenditure survival survival per head (5-year) (5 year) (2009 US$) Low income The Gambia 12% 22% 57 330 22 Uganda 46% 13% 52 370 28 India 52% 46% 65 990 40 Lower-middle income 47% 37% 74 1460 63 Philippines 82% 67% 75 2490 108 China 63% 61% 72 3240 136 Thailand Upper-middle 70% 53% 81 5530 488 income 77% 63% 74 8090 465 Costa Rica Turkey 79% 79% 83 21210 1362 High income 76% 66% 83 34640 1148 South Korea Singapore Health-care and economic data for ten countries by World Bank country income classification levels and 5-year survival for breast and cervical cancer. B. Anderson et al., Lancet Oncology 2011; 12:387-98
Survival of children with cancer in economically developed countries and in low-income countries
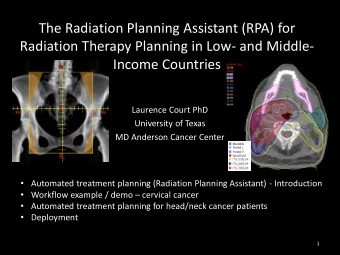
Access to Radiotherapy IAEA$has$ini*ated$PACT$to$ comprehensively$address$this$urgent$ problem,$and$is$moving$its$ radiotherapy$programmes$to$a$public$ health$model.$$
Cancer Drugs versus Cancer 16% 60% 5% 18% 5% 17% 18% 61%
The 5/80 Cancer Disequilibrium About 5% of global resources spent in low and middle income countries which account for almost 80% of the disability-adjusted life-years lost worldwide to cancer. Sloanza, Gelband H eds. Cancer control opportunities in low- and middle-income countries. Washington D.C.: Institute of Medicine of the National Academies, National Academies Press; 2007
The looming disaster in developing countries Sum of ! mainly poverty-related tumors (cervical, oesophagus, liver) ! tumors linked to western style of life (breast, lung, prostate, colorectal) ! lack of primary and secondary prevention ! lack of resources for treatment F. Cavalli. Nature Clinical Practice Oncology 2006; 11:582
Figure Correlation between government health expenditure and pediatric cancer survival Annual&government&spending&on&health&care&per&capita&($US)& R. Ribeiro et al. Lancet Oncology 2008; 9-721-729
Structure and efficiency of health care system KEY for the fight against cancer
“Universal health coverage is fundamental to improving the lives of people” Peter Anyang Nyong Kenia’s Health Minister Lancet 2012; 379:494
Current evolution (I) Anglophone sub-Saharian African Countries have seen 30 years of undermining of their health systems by structural adjustement and successive fiscal crises, contributing to wholesale emigration of trained health workers.
Current evolution (II) Many Asian and Latin-American health systems are tiered and fragmented because of the unregulated growth of private health care and successive externally-driven initiatives.
Current evolution (III) Public health systems in the countries of the former Soviet Union, previously universally accessible -albeit often inefficient- have been disrupted by reductions in funding and rapid privatization. Health systems strengthening: current and future activities. J. Sundvall et al. Lancet 377:1222-24; 2011
Current evolution (IV) Explosion of cost of systemic treatment, even for old drugs (e.g. Thalidomide, Thiotepa, etc.) (US prize is determinant) Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS) has “exacerbated the problem with no gain for developing countries R. Smith. Lancet 2009; 373:684-91
What to do? (I) (Tobacco " Africa) ! Prevention! Enforce FCTC ! Early detection adapted to local situation e.g. BGHI Cancer in developing countries: can the revolution begin? Lancet Oncology 2011; 12:201
What to do? (II) Palliative: ! twinning ! essential drugs (WHO) ! UNIQUE ! vertical programs (???) Curative: ! change of rules!
1086: La Mascota Project 150-200 USD/year Long-term twinning global-program ! training and supervision of helath professionals ! building inpatients - outpatients structures and laboratories facilities ! use of protocols tailored to the local possibilities ! clinical research ! use of part of resources for social help (Lost to therapy # ) Lancet 1998; 352:1923-26
Expansion of cancer care and control in countries of low and middle income: a call to action 3 examples: ! international partnership ! inclusion in national incurance programs ! expansion through a national center of excellence P. Farmer et al. Lancet 2010; 376:1186-93
UN SUMMIT on NCDs (19-20 September 2011) Additionally, the Declaration clearly acknowledges cancer as a unique disease in many respects, with specific commitments to prevention and early detection. We welcome commitments to: ! Give greater priority to early detection, screening and diagnosis of NCDs including cancer screening programs (particularly breast and cervical cancer) ! Increase access to Hepatitis B and HPV vaccines as part of national immunization programs to prevent infection-related cancers.
UN SUMMIT on NCDs (19-20 September 2011) However, there remain some areas where commitments fall short of expectations. The Declaration lacks specific targets including no overall goal of reducing preventable deaths. More work is now needed to convince governments around the world to commit to reduce the avoidable deaths from NCDs by 25% by 2025 - a target WHO believes to be achievable. In addition, there are no commitments to increase the proportion of development assistance devoted to health outcomes.
New WHO Resolutions 1. To reduce NCD-mortality in people <70 yrs by 25% till 2025 2. To prepair second Framework Convention (first FMCT) devoted to RD, mainly related to low income countries. ! 0.01% of BIP to be devoted. Geneva, May 25 th , 2012
Changes of rules ! abandon principle of patents ! compensate industry for discovery ! most of research ( F I ! III) to be financed by public resources. J. Stieglitz. blog “Project Syndicate”
Next steps 27-28 October 2012, Lugano, Switzerland: World Oncologic Forum (WOF) (Are we winning the war on cancer?)
Thank you
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries