
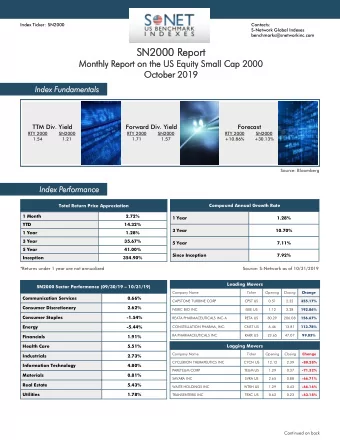
C ase r eport Glass displaced into the infratemporal region from - PDF document
Surgery Oral & Cranio-Maxillofacial Page 1 of 3 C ase r eport Glass displaced into the infratemporal region from submandibular injury: case report Z Hamdoon 1 , W Jerjes 1,2,3 *, RM Al-Delayme 1 , T Upile 2 , C Hopper 1,2 Abstract bar
Surgery Oral & Cranio-Maxillofacial Page 1 of 3 C ase r eport Glass displaced into the infratemporal region from submandibular injury: case report Z Hamdoon 1 , W Jerjes 1,2,3 *, RM Al-Delayme 1 , T Upile 2 , C Hopper 1,2 Abstract bar holding a wine glass. She fell onto the tuberosity to provide a wide exp - Introduction the glass. On physical examination, the osure of the fragment. The pterygoid This report describes glass displaced patient was presented with a 1.5 cm process was trimmed whilst prese - into the infratemporal region from laceration in the submandibular rving the coronoid process. submandibular injury. region. The buccal mucosa was normal To allow maximum sensitivity and Case Report without any signs of tearing or fistula. control, the surgeon performed a fin- This report describes an unusual cas- The wound was cleaned, debrided and ger dissection to facilitate the move- All authors contributed to the conception, design, and preparation of the manuscript, as well as read and approved the final manuscript. e with foreign body displacement fr- sutured. The patient was kept under ment of the fragment through various om submandibular region to infrate- observation in the hospital for 12 anatomic spaces, starting from below mporal fossa. An appropriate surgic- hours and discharged with a Glasgow and moving upward. The pathway of al approach to retrieve the object us- Coma Scale (GCS) of 15. In the follow- egress was mapped by keeping close ing a trans-oral approach is disc- up clinic, the patient reported swelling, to the lateral pterygoid plate and then ussed. pain, and impaired mouth opening for moving along the lateral surface of Conclusion over 2 days after the discharge. the medial pterygoid muscle toward Cross-sectional scanning detected a Retrieving a foreign body in the ITF the lateral pterygoid muscle. Extreme moderately dense irregular mass located using an intro-oral approach should care was taken to avoid an inferior in the infratemporal fossa (ITF). The be guided by the precise location and alveolar nerve injury. thickness (1 mm) and shape of the mass size of the object, the signs and sym- The Howarth periosteal elevator is suggested a glass fragment. The glass ptoms presented by the patient, and used transorally, both for exposure fragment superiorly extended to the the surgeons knowledge and skill. and haptic feedback. Once the intraor- skull base and sphenoid sinus, inferiorly al elevator palpated the fragment, int- to the level of para-pharyngeal space Introduction estinal clamping forceps clamped the and anteriorly to the lateral pterygoid Many surgical approaches have been fragment whilst avoiding the local soft process. All authors abide by the Association for Medical Ethics (AME) ethical rules of disclosure. suggested in the literature to recover tissue. The fragment was gently remo - In the Head and Neck Trauma Multi- a foreign body displaced into the ITF, ved with malleable copper retract - Discipline meeting (MDM), discussion such as long incision in the buccal su- ors placed medially to the fragment about leaving or removal of the glass lcus, Caldwell–Luc approach through to protect the vasculature during ma - fragment was raised, with final the maxillary sinus after removal of noeuvring (Figure 1). By 2 weeks consensus decision toward operative Competing interests: none declared. Conflict of interests: none declared. the whole posterior wall and resecti- postoperatively, the patient fully exploration and removal. This was on of the coronoid process 1 . We rep- recovered, without adverse sequel. predicated on the following factors: a ort an unusual case with foreign bod- high-risk location with proximity to y displacement from submandibular Discussion the maxillary artery and size of the region to infratemporal fossa. In our case, the glass fragment (for- object (2 × 2 cm) and facial weakness. eign body) was displaced at the lower The glass fragment was Case Report part of the ITF; therefore, an intraoral successfully removed via a trans- An 18-year-old intoxicated female approach using partial maxillectomy tuberosity approach under general was admitted to our hospital at the (tubersectomy) was chosen, which anaesthesia. A vertical incision was A&E department after falling in the showed satisfactory results without made starting in the gingivolabial any additional procedure. This ap- sulcus posteriorly, close to the max - * Corresponding author proach has 3 advantages: (1) it offers illary tuberosity, and then extended Email: waseem_wk1@yahoo.co.uk a good cosmetic result without obvious to the retro-molar area and proceed - 1 Unit of Oral and Maxillofacial Surgery, UCL scarring (2) it provides adequate expo- ing down to the mandibular ridge, Eastman Dental Institute, London, UK 2 Department of Surgery, UCL Medical School, sure and (3) it protects the facial nerves. then along the ascending ramus London, UK Acute removal of fragments is easier towards mandibular angle. An 3 Leeds Institute of Molecular Medicine, and less hazardous than at a later osteotomy was performed in the University of Leeds, Leeds, UK Licensee OA Publishing London 2012. Creative Commons Attribution License (CC-BY) F�� �������� ��������: Hamdoon Z, Jerje s W , Al-De layme RM, Upile T , Hopper C. Glass displaced into the infratemporal region from submandibular injury: a case report. Hard Tissue. 2012 Nov 10;1(1):6.
Page 2 of 3 C ase r eport stage, when adhesion of normal ana- (A) (B) tomic planes by fibrous tissue as well as fragment encapsulation by fibrous tissue takes place. The size of the for- eign body was a factor in the decision for or against its removal. Removal of small shell fragments (≤1 cm in diam- eter) is considered when surgical damage is determined to be minimal; (C) (D) if not, they are left alone. Irregular shape, deformation, hooks, multiple edges and position increase the number of expected com- plications during surgery. Shuker 2,3 All authors contributed to the conception, design, and preparation of the manuscript, as well as read and approved the final manuscript. discussed projectile retrieval of high risk bullets/fragments lodged in the sphenoid sinuses and ITF. This injury has a high potential for infection and (E) (F) more complications in the ITF, be- cause along its pathway, the projectile may carry with it a bone or tooth frag- ments that are frequently observed in its course and around the shell. Malignant processes have been reported in conjunction with the pro- longed presence of a foreign body 4 . Cases of delayed aneurysm and abscess (G) (H) at the site of a retained foreign body 5 as well as foreign body granulomas and reactions have been described 6 . In addi- tion, there remains a possibility of late All authors abide by the Association for Medical Ethics (AME) ethical rules of disclosure. infection and erosion of the vessel walls in this dangerous region. Moreover, the patients’ fears may result in psychologi- cal consequences 7,8 . (I) (J) These arguments support the need Competing interests: none declared. Conflict of interests: none declared. for an early removal of foreign bodies whenever possible. Foreign bodies in the head and neck are occasionally difficult to manage even when a plan has been formulated from static pre- operative images. The surgeon should be prepared for unpredictable com- plications, such as haemorrhage, and Figure 1: (A) Para-sagittal CT view showing the relation of the glass fragment pre-emptively consider an alternative (foreign body) to the pterygoid plate, skull base and cervical vertebrae. surgical approach. (B) Axial CT view of the same foreign body. (C) The patient being prepped prior In this case report, a trans-oral ap- to extraction of the foreign body; the wide submandibular scar indicated the proach was found to be the safest way to entry site of the foreign body. (D) Intraoral view of the left upper buccal space— retrieve the foreign body. Using a sub- the site of surgical entry. (E) Incision through the left upper buccal mucosa and mandibular approach, utilizing the entry bone exposure. (F) Bone window opened with an aim to identify the location path of the foreign body was not feasible of the foreign body. (G) Extraction of the foreign body in process. (H) Foreign because of adjacent vital structures. body removed (glass). (I) Closure of the buccal mucosa after appropriate For removal (extraction), the for- debridement. (J) Final image of the foreign body after extraction. eign body should be localized exactly Licensee OA Publishing London 2012. Creative Commons Attribution License (CC-BY) F�� �������� ��������: Hamdoon Z, Jerje s W , Al-De layme RM, Upile T , Hopper C. Glass displaced into the infratemporal region from submandibular injury: a case report. Hard Tissue. 2012 Nov 10;1(1):6.
Recommend
![[1] Defini=on of allele-specific expression (ASE) Adopted from Unneberg, 2010 One gene can](https://c.sambuz.com/709481/1-defini-on-of-allele-specific-s.webp)





More recommend
Explore More Topics
Stay informed with curated content and fresh updates.