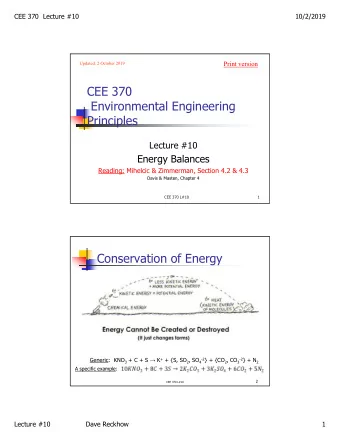
9/21/2015 BATTLEFIELD ANESTHESIA PATRICIA WEOTT DNAP CRNA MAJ USAR I have no disclosures 1
9/21/2015 OBJECTIVES • Describe the goals of anesthesia in a combat zone • List the components of a Forward Surgical Team • Describe available assets to perform anesthesia in a battle zone • Discuss the hardships of living in an austere environment 2
9/21/2015 Irony of War • Civil/ WWI : Anatomy books • WW II: Mobile units referred to as the “Trinity” comprised of neurosurgeons, plastic surgeons and ophthalmic surgeons. First experience with psychosomatic/conversion disorders R/T Battlefield Trauma (PTSD). • Korea: First Air Ambulance • Vietnam: Huey Helicopters for evacuation, medical corpsmen: surgical airways, needle decompressions and shock resuscitation; which led to our modern system of prehospital emergency care via EMTs and paramedics. MASH Units, ‘Golden Hour of Care’. Persian Gulf Wars: Mobile Intensive Care Units, Blood Transfusion 1:1:1. Signature Injuries • Vietnam: PTSD/ Agent Orange • Iraq: Amputations • Afghanistan: Closed Head Injuries and Concussions 3
9/21/2015 PREVENTABLE CAUSES OF COMBAT DEATH • 60% Hemorrhage from extremity wounds • 33% Tension pneumothorax • 6% Airway obstruction e.g., maxillofacial trauma 4
9/21/2015 5
9/21/2015 Signature Injury: Blast/CHI 6
9/21/2015 Primary Blast Injury • An explosion generates a blast wave traveling faster than sound and creating a surge of high pressure immediately followed by a vacuum. The blast wave shoots through armor and soldiers' skulls and brains. While the exact mechanisms by which it damages the brain's cells and circuits are still being studied, the blast wave's pressure has been show to compress the torso, impacting blood vessels, which then send damaging energy pulses into the brain. The pressure can also be transferred partially through the skull, interacting with the brain. 7
9/21/2015 Airway • According to TCCC guidelines, surgical cricothyroidotomy is the preferred method for establishing a definitive airway during tactical field care or the tactical evacuation phase. This assumes care ‐ providers in the field lack the necessary equipment, pharmaceutical agents, or training to perform rapid ‐ sequence orotracheal intubation. CPGs • Clinical Practice Guidelines • Evidence ‐ based • Improves care by reducing variation in practice and systematizing “best practices”. • Serve to reduce errors and provide consistent quality of care. • Guidelines also are cornerstones for accountability and facilitate learning and the conduct of research. 8
9/21/2015 FORWARD SURGICAL TEAM 9
9/21/2015 SPECIAL FORCES aka ODA/ODB • 18A Team Leader • 18Z Team Sergeant • 18A Warrant Officer • 18B Weapons • 18C Engineer • 18D (Delta) Medic • 18E Communications • 18F Intel 10
9/21/2015 11
9/21/2015 12
9/21/2015 Lethal Triad • Hypothermia • Coagulopathy • Acidosis 13
9/21/2015 Care Under Fire (cont.) • Return fire as directed or required • If able, the casualty(s) should also return fire • Try to keep from being shot • Try to keep the casualty from sustaining additional wounds • Airway management is best deferred until the Tactical Field Care phase • Stop any life threatening hemorrhage with a commercially available tourniquet (CAT) • Reassure the casualty 14
9/21/2015 Challenges of Deployments • Absolute Isolation • Personnel with deployment stress and loaded weapons • Supplies • Weather • “Groundhog Day” • Embedded with Afghans/Iraqis • Flashbacks 15
9/21/2015 16
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries