Acute and Midterm Outcomes of the AMDS Arch Remodeling Therapy: - PowerPoint PPT Presentation
Acute and Midterm Outcomes of the AMDS Arch Remodeling Therapy: DARTS Prospective International Trial STS 56 th Annual Meeting Dr. Michael C. Moon Mazankowski Alberta Heart Institute University of Alberta Edmonton, Alberta, Canada
Acute and Midterm Outcomes of the AMDS Arch Remodeling Therapy: DARTS Prospective International Trial STS 56 th Annual Meeting Dr. Michael C. Moon Mazankowski Alberta Heart Institute University of Alberta Edmonton, Alberta, Canada
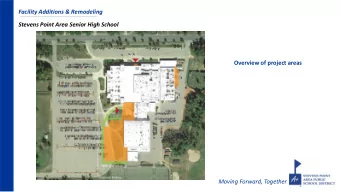
Background: Today’s Gap • Today’s standard -of-care hemiarch repair successfully addresses the primary entry tear by resection, however, there are significant limitations: 1. Potential creation of a distal anastomotic new entry (DANE) tear(s) , allowing for antegrade pulsatile flow (APF) and pressurization of the FL 2. Lack of predictable and reliable visceral and peripheral malperfusion resolution reflected in the high mortality and reinterventions associated with malperfusion.
What Causes the Pressurized FL? Negative Remodeling • Friability of the dissected aorta, results in 50-70% a DANE which as a Primary Entry Tear (PET). • Pressurization of the FL via the PET (Primary Entry Tear) leads to TL collapse, malperfusion and Distal aortic growth primarily in the Anastomotic region adjacent to the PET. New Entry ( DANE ) * Malperfusion Bing F, et al. Vascular and Endovascular Surgery 2014;48(3): 239-245 Yasuda S, et al. Circ J doi: 10.1253/circj.CJ-16-0462 Tamura K, et al. Eur J Cardio-Thorac Surg 2017;(52): 867 – 873 Rylski B, et al. Eur J Cardio-Thorac Surg 2017:(51):1127-1134
AMDS: Mode of Action • Bridges the treatment gap • Maximize the benefits of today’s standard of care without adding complexity • Supported seal cuff • Effective sealing of the DANE • Uncovered stent component • Allows for uninhibited flow to arch vessels and other aortic branches • Enables min. inv. re-interventions if necessary
The AMDS Hybrid Prosthesis: Biluminal Management • Minimize development of a DANE at the distal TL anastomosis, abolish the APF, Expansion decrease the flow into and Zone: Malperfusion depressurizing the FL. Management • Expansion, maintenance and pressurization of the TL improves end-organ Seal Zone: circulation and manages Stent Supported Cuff for FL maplerfusion. Management
DARTS Trial: Objective and Enrollment • To analyze the safety and performance of the AMDS device at midterm follow-up in patients presenting with acute DeBakey I aortic dissection undergoing surgical repair. • The largest prospective, monitored ATAD device trial to date. • Inclusion Criteria • Patients 18-80 years • Acute DeBakey I aortic dissection within 14-days • Exclusion Criteria • Extreme hemodynamic compromise requiring CPR • Marfan, Loeys-Dietz, or Ehlers-Danlos syndrome • Proximal descending thoracic aortic aneurysm >45mm
Study End-Points • Primary: All-cause mortality and SAEs at 30-day SAEs: neurologic dysfunction, device-related adverse outcomes • Secondary: Malperfusion resolution Aortic remodelling FL response and status All-cause mortality and SAEs at 1 year
Aortic Zone Analysis
Demographics • From March 2017 to January 2019, a total of 47 patients underwent emergent surgical repair with AMDS implantation • One patient was excluded from all analysis due to implantation of an AMDS in an iatrogenic dissection during a mitral valve repair Baseline Characteristic % (n=46), Value (IQR) Age (y) 62.5 (48.5, 70.8) Male gender 67.4% (n=31) Malperfusion 56.5% (n=26) Reoperation 4.3% (n=2) Hypertension 63.0% (n=29) Chronic renal failure 13.0% (n=6) COPD 13.0% (n=6) Pre-operative stroke 19.6% (n=9)
Procedure and Hospital Course Characteristic % (n=46), Value (IQR) Successful device deployment 100% (n=46) Hemiarch repair 97.8% (n=45) Total arch replacement 2.2% (n=1) Aortic root replacement 45.7% (n=21) Median DHCA duration (min) 33.5 (26.0, 41.5) Median cerebral perfusion duration (min) 30.5 (23.0, 37.8) Median AMDS implantation time (min) 3.0 (2.0, 5.0) Median ICU length-of-stay (days) 6.0 (4.0, 12.0) Median hospital length-of-stay (days) 13.0 (8.0, 18.0) Blood transfusion required 60.9% (n=28) Median number of units transfused within 24-hours 3.0 (2.0, 6.0)
Mortality and Serious Adverse Events Mortality and Serious Adverse Events % (n=46), Value (IQR) Mortality 30-day 13.0% (n=6) 1-year 19.6% (n=9) Aorta-related 0% (n=0) Malperfusion-related 7.7% (2/26) New stroke 30-day 6.5% (n=3) 1-year 6.5% (n=3) Spinal cord ischemia 0% (n=0) Acute renal failure requiring dialysis 10.9% (n=5) Aortic injury associated with device implantation 0% (n=0) Stent fracture 0% (n=0) Distal stent-induced new entry tear 0% (n=0) Device-related reintervention 0% (n=0)
Mortality Freedom from Overall and Aorta-Related Mortality 1 0.8 0.6 S (t) 0.4 0.2 Overall Mortality Aorta-Related Mortality 0 0 200 400 600 800 1000 1200 Surival Time (t) Days Time Post-Treatment (Days) Number of Subjects at Risk 0 46 30 40 365 37 545 26 730 8 1000 1
Malperfusion Management • 95.5% (n=63) of vessel malperfusions resolved after AMDS implantation, without a secondary procedure • 100% (n=3) of patients presenting with spinal cord ischemia manifesting as paralysis had complete reversal of their paralysis post-operatively • Cerebral malperfusion involving the supra-aortic vessels (SAVs) was anatomically resolved in 85.7% (18/21) of the vessels involved.
Aortic Remodeling B1 B2 B3 C Aortic Zone A Change from Baseline** % (N=35*), % (N=35*), % (N=35*), % (N=35*), % (N=35*), (n/N) (n/N) (n/N) (n/N) (n/N) Total Aortic Diameter 8.6 (3/35) 2.9 (1/35) 0.0 (0/35) 2.9 (1/35) Decrease 34.3 (12/35) 68.6 (24/35) 77.1 (27/35) 80.0 (28/35) 71.4 (25/35) Stable 65.7 (23/35) 22.9 (8/35) 20.0 (7/35) 20.0 (7/35) 25.7 (9/35) Increase 0.0 (0/35) TL Diameter 0.0 (0/35) 0.0 (0/35) 0.0 (0/35) 0.0 (0/35) Decrease 0.0 (0/35) 14.3 (5/35) 31.4 (11/35) 22.9 (8/35) 51.4 (18/35) Stable 11.4 (4/35) Increase 88.6 (31/35) 82.9 (29/35) 65.7 (23/35) 74.3 (26/35) 45.7 (16/35) FL Diameter Decrease 88.6 (31/35) 88.6 (31/35) 40.0 (14/35) 54.3 (19/35) 25.7 (9/35) 8.6 (3/35) 34.3 (12/35) 31.4 (11/35) 51.4 (18/35) Stable 11.4 (4/35) Increase 0.0 (0/35) 2.9 (1/35) 22.9 (8/35) 11.4 (4/35) 20.0 (7/35) *35 patients have at least 1-year follow-up CT compared to the 1 st post-operative CT scan as a baseline **Maximum diameter measured
False Lumen Response B1 B2 B3 C Aortic Zone A % (N=34 # ), % (N=34 $ ), False Lumen % (N=39*), % (N=38**), (N=36***), Response (n/N) (n/N) (n/N) (n/N) (n/N) 26.3 (10/38) 11.1 (4/36) 2.9 (1/34) 2.9 (1/34) Obliterated 61.5 (24/39) 26.3 (10/38) 19.4 (7/36) 20.6 (7/34) 11.8 (4/34) Completely 12.8 (5/39) thrombosed Partially thrombosed 10.3 (4/39) 15.8 (6/38) 36.1 (13/36) 32.4 (11/34) 44.1 (15/34) 31.6 (12/38) 33.3 (12/36) 44.1 (15/34) 41.2 (14/34) Patent 15.4 (6/39) *39 patients have at least 1 follow-up CT and latest CT scan was used for analysis compared to the 1 st post-operative CT scan as a baseline **One dissection ended in distal arch ***Two dissections ended in proximal descending # Two dissections ended in the mid/distal descending
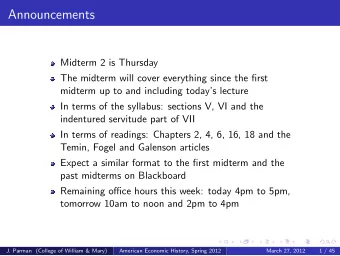
D E Nearly Occluded Patent Common Carotid Common Arteries Carotid Arteries G F Occluded Patent SMA SMA Patent Renal Occluded Renal Arteries Arteries Bilaterally Bilaterally
Courtesy University Hospital Network, Toronto
Secondary Procedures • Three patients (6.5%) required malperfusion-related secondary procedures • Left renal artery stenting for static malperfusion • Superior mesenteric artery stenting for static malperfusion • Left common carotid artery stenting due to de-novo dissection of the carotid artery distal to origin of the vessel • One patient (2.2%) require an aortic growth-related secondary procedure • Left common carotid interposition graft, left subclavian covered stent and coiling of the FL • No reintervention was directed towards the aortic arch
Secondary Procedures Freedom from Malperfusion-Related and Aorta-Related Reintervention 1 0.8 0.6 S (t) 0.4 0.2 Malperfusion-Related Aorta-Related 0 0 200 400 600 800 1000 1200 Surival Time (t) Days Time Post-Treatment (Days) Number of Subjects at Risk 0 46 30 40 365 37 545 26 730 8 1000 1
Conclusion • The DARTS trial results support the use of the AMDS Hybrid Prosthesis as a safe and effective treatment for acute DeBakey I dissections. • Effective sealing of the FL at the distal anastomosis with the AMDS was achieved in 90% of the patients. This seal together with TL expansion leads to elimination of the APF into the FL and improved perfusion of the TL. • The AMDS complements the standard-of-care procedure and can improve survival, provide effective and reliable management of malperfusions, induce positive aortic remodeling and reduce the reintervention rates involving the aortic arch.
Questions?
Recommend








More recommend
Explore More Topics
Stay informed with curated content and fresh updates.