4/18/19 Thomas and Cherney (2018) Diabetologia DOI - PDF document
4/18/19 Thomas and Cherney (2018) Diabetologia DOI 10.1007/s00125-018-4669-0 SGLT-2 Inhibition Effect On eGFR Class effect : initial drop in eGFR ~ 5 mL/min/ 1.73/m followed by stabilization Effect observed in eGFR as low as 30 ml/min
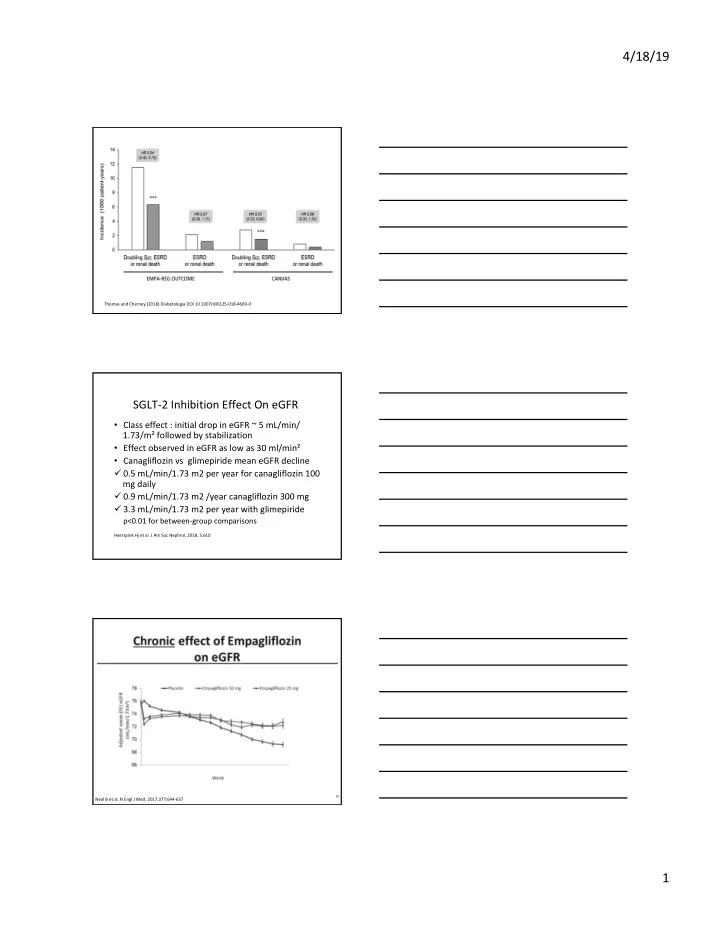
4/18/19 Thomas and Cherney (2018) Diabetologia DOI 10.1007/s00125-018-4669-0 SGLT-2 Inhibition Effect On eGFR • Class effect : initial drop in eGFR ~ 5 mL/min/ 1.73/m² followed by stabilization • Effect observed in eGFR as low as 30 ml/min² • Canagliflozin vs glimepiride mean eGFR decline ü 0.5 mL/min/1.73 m2 per year for canagliflozin 100 mg daily ü 0.9 mL/min/1.73 m2 /year canagliflozin 300 mg ü 3.3 mL/min/1.73 m2 per year with glimepiride p<0.01 for between-group comparisons Heerspink Hj et al. J Am Soc Nephrol, 2018, 5:610 30 Neal B et al. N Engl J Med, 2017;377:644-657 1
4/18/19 Effects of Canagliflozin on eGFR in DM 2 and DKD stage 3 ( mean eGFR 40 ml/min; UACR > 30 mg/g) Concurrent decrease in body weight (~ 1 kg) and systolic blood pressure (~ 6 mm Hg) at 100 and 300 mg dose Yale JF et al. Diabetes and Metabolism 2013; 15: 463-473463 SGLT-2 Inhibition Effect on Albuminuria • 38% reduction in EMPA-REG • CANVAS showed 27% reduction in progression to severe albuminuria and 1.7- fold higher regression • 36% dapa decreased 24-hour urine secretion • Effect preserved in eGFR ≥30 to <50 ml/ min/1.73 2 ( cana vs. glimepiride) Heerspink HJ et al. J Am Soc Nehprol 2017; 28:368 Neal B et al. N Engl J Med 2017;377:644-657 Wanner C et al. N Engl J Med. 2016;375:323 Putative mechanism (Indirect Mechanism) 1. Blood glucose-lowering effect 2. Blood pressure reduction is class effect , decrease in systolic and diastolic blood pressure by ~2 and ~ 5 mmHg amplified in CKD patients : -3.2 mmHg in eGFR > 90; -4 mmHg in 60-89; -6.6 mmHg in eGFR < 30 ml/min/1.73m² • 2-3 kg weight loss within 6 months of initiation of treatment, preserved after 2 years of treatment with dapagliflozin, preserved in eGFR as low as 30 ml/min/1.73m² Cherney DZ et al. Kidney Int 2018; 93:231 Thomas MC et al. Diabetologia 2018; 61:2098-2107 33 2
4/18/19 Effects of Canagliflozin on Glycated Hemoglobin Level, Body Weight, and Systolic and Diastolic Blood Pressure in the Integrated CANVAS Program. Neal B et al. N Engl J Med 2017;377:644-657 l B et al. N Engl J Med 2017;377:644-657. A. Diabetic nephron B. Diabetic nephron with SGLT inhibition Tubular Tubular ATP cleavage epithelial cell ATP cleavage epithelial cell Adenosine activation Adenosine activation to adenosine to adenosine of (A 1 ) receptor of (A 1 ) receptor Basolateral Basolateral ATP release ATP release [Ca 2+ ] 3 Na + ATP [Na + ] Tubular [Ca 2+ ] 3 Na + ATP [Na + ] Tubular Vaso- [K + ] Vaso- [K + ] 2 K + H 2 O lumen lumen constriction ADP + P i [Cl - ] dilation 2 K + ADP + P i H 2 O [Cl - ] Na + /K + - Na + /K + - Afferent arteriole ATPase ATPase Afferent arteriole reduced high P GC feedback from increased feedback from macula reversed macula densa afferent afferent densa normalized vasodilation vasodilation P GC increased NaCl and glucose filtration increased NaCl and glucose reabsorption via SGLT-2 decreased NaCl and glucose reabsorption via SGLT-2 inhibition normalized decreased distal delivery distal delivery of NaCl of NaCl Sodium-glucose co-transporter-2 (SG LT-2) Sodium-glucose co-transporter-1 (SG LT-1) Sodium (Na) Chloride (Cl) Glucose P GC = pressure in glomerular capillary Adapted from Alicic et al., Diabetes 2019; 68: 248-257 Putative mechanisms (Direct effects) • Hemodynamic effect– normalization of hyperperfusion , hyperfiltration and glomerular hypertension • Metabolic effect: • anti-inflammatory • antifibrotic effect • effect on tubular hypoxia Thomas MC et al. Diabetologia 2018; 61:2098-2107 Alicic RZ et al. Diabetes 2019;68:248–257 | 3
4/18/19 Scheen AJ. Circ Res 2018; 122:1439 SGLT-2 and NHE3 crosstalk and effects of SGLT2 inhibition • Decreased inflammation and oxidative stress • Reduction of necrosis and fibrosis • Improved endothelial function and vascular compliance Verma S. et al. Diabetologia, 2018; 61:2108-2125 Role and regulation of intestinal SGLT1 for glucose uptake and potential therapeutic applications of SGLT1 inhibitors ( Gut) Rieg and Vallon (2018) Diabetologia DOI 10.1007/s00125-018-4654-7 39 4
4/18/19 SGLT1 inhibition • Predominantly reduces glucose absorption in the proximal intestine, which significantly blunts and delays postprandial hyperglycemia • Small effect of glucose reabsorption in the kidney • SGLT1 role in etiology of cardiomyopathy unclear Powell DR, et al. Am J Physiol Endocrinol Metab 2013; 304:E117–E130 40 Song P et al. Expert Opin Ther Targets 2016; 20:1109-1125 SGLT inhibitors adjunct therapy in DM 1 • Placebo-controlled phase II trials with empagliflozin (EASE-1), canagliflozin, dapagliflozin and sotagliflozin conducted in 2014 and 2015 • Phase III trials ( DEPICT-1 and 2, TANDEM1,2,3, EASE-2) • Demonstrated average effect : ü 0.4-0.5 % reduction in HbA1c ( 5-6 mmol/mol) ü 10-15% Reduction in daily insulin dose; reduction in glucose excursions ü 3-4 kg weight loss ü No increase in rates of hypoglycemia McCrimmon RJ et al. Diabetologia,2018;61:2126-2133 41 Effects of Sotagliflozin Added to Insulin in Patients with Type 1 Diabetes (TANDEM3) -The reduction in body weight greater in the sotagliflozin group than in the placebo group (difference, −2.98 kg; P<0.001) -Reductions from baseline in the mean daily total, bolus, and basal doses of insulin were −5.3 units per day (−9.7%), −2.8 units per day (−12.3%), and −2.6 units per day (−9.9%) ( P <0.001 ) - The reduction in systolic blood pressure was significantly greater in the sotagliflozin group than in the placebo group (difference, −3.5 mm Hg; P=0.002) Garg SK et al. N Engl J med 2017;377:2337-2348 42 5
4/18/19 Side Effects of SGLT2 inhibitors • Genital mycotic infections • FDA warning: DKA ( in DM1 and DM2 patinets) • 2013 – 2015 reported 73 cases • FDA warning: Fournier’s gangrene • 2013 – 2018 reported 12 cases • Initial concern for AKI and hyperkalemia not observed in large trials • Low risk of hypoglycemia • Lower extremity amputations (cana) Comparison of Rates of Diabetic Ketoacidosis in DEPICT-1 and in Tandem3 Trials after Standardization of the Criteria Used Garg S and Strumph P. N Engl J Med 2018;378:966-968 . Risk of Diabetic Ketoacidosis after Initiation of an SGLT2 Inhibitor Fralick M et al. N Engl J Med 2017;376:2300-2302 . 6
4/18/19 TANDEM3 trial • The number need to treat to show benefit is 7 • The numbers of patients who would need to be treated with sotagliflozin to show harm from at least: ü one episode of severe hypoglycemia 167 ü diabetic ketoacidosis 40 ü volume depletion 64 ü genital mycotic infection 23 Gogtay NT et al. N Eng J Med 2018;378:966 McCrimmon RJ et al. Diabetologia,2018;61:2126-2133 Lower extremities amputations • Observed in the CANVAS program (6 vs 3 participants per 1,000 years ; HR 1.97) • The highest risk among patients with PVD and h/o amputations majority at the toe/metatarsal level • Canagliflozin labeling changed in 2017 • Not reported with empa-or dapagliflozin 7
Recommend









More recommend
Explore More Topics
Stay informed with curated content and fresh updates.