
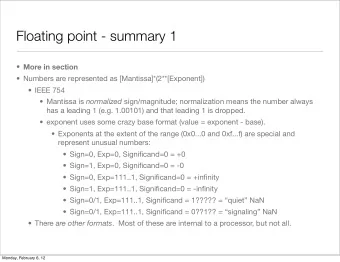
1 Definition Clinical diagnosis is by either. Disorder - PDF document
Objectives Review osteoporosis risk assessment: A Bone to Pick: Osteoporosis Risk Guidelines Assessment Controversies Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA The Situation 1 in
Objectives Review osteoporosis risk assessment: A Bone to Pick: Osteoporosis Risk Guidelines Assessment Controversies Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA The Situation 1 in 2 postmenopausal women will have an osteoporosis-related fracture in their lifetimes!! Because of the aging of the U.S. population, the number of hip fractures in the U.S. is expected to double or triple by 2040. Direct medical care costs of osteoporotic fractures = (USPSTF, Ann Intern Med 3/1/2011, Schneider and Guralnik 1990, Wright et al $17 billion/yr U.S. JBMR 2014) (USPSTF 2011, Blume & Curtis OI 2011) 1
Definition Clinical diagnosis is by either…. Disorder characterized by low bone mass and microarchitectural Adulthood hip or vertebral fracture in the absence of major trauma (such as deterioration of bone tissue, leading to enhanced bone fragility and a motor vehicle accident of multiple story fall)---regardless of BMD value!! consequent increase in fracture risk. or BMD T-score ≤ -2.5 at lumbar spine or hip by dual-energy x-ray absorptiometry (DXA) (National Osteoporosis Foundation Clinician’s Guide to Prevention and Treatment of Osteoporosis 2014 www.nof.org, Amer. Assoc. Clin. (Consensus development conference: diagnosis, prophylaxis and treatment of Endocrinologists 2010) osteoporosis, Am J Med 1993 & WHO Technical Report Series 843, Geneva 1994, Surgeon General’s Report on Bone Health and Osteoporosis 2004) World Health Organization Diagnostic class. Which test? Classification BMD T-score Normal Within 1 SD of a young adult T-score at -1.0 and Current diagnostic and treatment criteria rely on dual- reference population above energy x-ray absorptiometry (DXA) measurements of Low Bone Mass Between 1.0 and 2.5 SD below T-score between lumbar spine and hip ONLY. (Osteopenia) that of a young-adult reference -1.0 and -2.5 population T-scores from other technologies cannot be used Osteoporosis 2.5 SD or more below that of a T-score at or below -2.5 according to the WHO diagnostic classification because young-adult reference they are not equivalent to T-scores derived from DXA. population Severe or 2.5 SD or more below that of a T-score at or below -2.5 (USPSTF Ann Intern Med 3/1/2011, National Osteoporosis Established young- adult reference with one or more Foundation Clinician’s Guide to Prevention and Treatment Osteoporosis population fractures of Osteoporosis 2014 www.nof.org, International Society (National Osteoporosis Foundation Clinician’s Guide to Prevention and Treatment of for Clinical Densiometry 2015) Osteoporosis 2014 www.nof.org & ISCD.org)(ref 20-29 y/o ♀ NHANES Looker et al 1998) 2
Which women to screen Whom to screen Women 65 years or older (USPSTF 2011, NOF 2014) Postmenopausal women aged 50-64: fracture during adulthood, or condition (e.g. rheumatoid arthritis) or medication associated with low bone mass or bone loss (NOF 2014) Women <65 y/o whose 10-year risk of osteoporotic fracture is ≥ that of a 65-year-old white woman who has no additional risk factors (i.e. ≥ 9.3%) (USPSTF) (USPSTF Ann Intern Med 3/1/2011, National Osteoporosis Foundation Clinician’s Guide to Prevention and Treatment of Osteoporosis 2014 www.nof.org) U.S. FRAX practical considerations FRAX in Not validated for spine bone mass 2016 If normal hip bone mass with low spine bone mass, FRAX underestimates fracture risk (version 3.10) Not validated for: Patients treated with osteoporosis pharmacotherapy past 1-2 years Underestimates fracture risk in patients with: Race- Recent or multiple fractures specific Those at increased risk for falling Outputs: 10-year prob. of hip fracture & 10-year BMD info prob. of major osteoporotic fracture (clinical (National Osteoporosis Foundation Clinician’s Guide to Prevention and Treatment of optional Osteoporosis 2014 www.nof.org) spine, forearm, hip or shoulder fracture) http://www.sheffield.ac.uk/FRAX/ 3
Controversy 1: Screening young Prior to advent of FRAX postmenopausal women United States Preventive Services Task Force (USPSTF) Osteoporosis Self-Assessment Tool (OST): weight, age (Cadarette 2004, Geusens 2002, Gourlay 2005, Lydick 1998) Women 65 years or older Simple Calculated Osteoporosis Risk Estimation Tool (SCORE): weight Women <65 y/o whose 10-year predicted risk of major osteoporotic age fracture is ≥ 9.3 % (65 year-old white woman no other osteoporosis race risk factors) rheumatoid arthritis non-traumatic hip, wrist, or rib fracture after age 45 years prior estrogen therapy (Lydick 1998) (USPSTF, Ann Intern Med 3/1/2011) Objective To compare, among postmenopausal U.S. women aged 50-64 years, the ability of the current USPSTF FRAX-based screening strategy with that of SCORE and OST to discriminate between women who did and did not experience incident major osteoporotic fractures over 10 years of f/u. No published studies had done this. (Crandall, et al J Clin Endocrinol Metab. 2014 Dec;99(12):4514-22. doi: 10.1210/jc.2014-2332. PMID: 25322268) 4
Sensitivity, specificity, and AUC values for identifying major Varying cutpoints to obtain sensitivity of ≥ 80% osteoporotic fracture (10 years of follow-up), stratified by age FRAX Sens (95% CI) Spec (95% CI) PPV (95% CI) AUC (95% CI) ≥ 4.81 80.1 (79.0-81.2) 28.7(28.3-29.1) 9.3 (9.0-9.6) 0.54 (0.54-0.55) ≥ 4.33 85.2 (84.2-86.1) 22.8 (22.4-23.1) 9.2 (8.9-9.4) 0.54 (0.53-0.54) ≥ 3.75 90.1 (89.3-90.9) 16.1 (15.8-16.4) 8.9 (8.7-9.2) 0.53 (0.53-0.54) ≥ 2.98 95.0 (94.4-95.6) 9.1 (8.9-9.3) 8.7 (8.5-8.9) 0.52 (0.52-0.52) ≥ 1.79 99.0 (98.8-99.3) 1.8 (1.7-1.9) 8.4 (8.2-8.7) 0.50 (0.50-0.51) SCORE > 2 81.0 (80.0-82.1) 22.0 (21.6-22.3) 8.7 (8.4-8.9) 0.52 (0.51-0.52) > 1 85.8 (84.9-86.8) 17.1 (16.8-17.4) 8.6 (8.4-8.9) 0.51 (0.51-0.52) > -1 91.7 (91.0-92.5) 10.2 (10.0-10.4) 8.5 (8.3-8.8) 0.51 (0.51-0.51) > -3 95.4 (94.8-95.9) 5.9 (5.7-6.1) 8.5 (8.3-8.7) 0.51 (0.50-0.51) > -9 99.0 (98.8-99.3) 1.2 (1.1-1.3) 8.4 (8.2-8.6) 0.50 (0.50-0.50) (Crandall, et al, J Clin Endocrinol Metab. 2014 99(12):4514-22) (Crandall et al, J Clin Endocrinol Metab. 2014 99(12):4514-22) Varying cut-points to obtain sensitivity ≥ Summary 80% Among women aged 50-64: OST Sens (95% CI) Spec (95% CI) PPV (95% CI) AUC (95% CI) < 6 80.6 (79.5 ‐ 81.7) 18.9 (18.5 ‐ 19.2) 8.3 (8.1 ‐ 8.6) 0.50 (0.50 ‐ 0.51) The USPSTF strategy only identified about one-quarter of women who < 7 86.5 (85.5 ‐ 87.4) 13.5 (13.2 ‐ 13.7) 8.4 (8.1 ‐ 8.6) 0.50 (0.50 ‐ 0.51) went on to experience incident fracture during 10-year follow-up. < 8 90.3 (89.5 ‐ 91.1) 9.6 (9.4 ‐ 9.8) 8.4 (8.1 ‐ 8.6) 0.50 (0.50 ‐ 0.50) The low sensitivity was especially apparent for the youngest women (ages < 10 95.1 (94.5 ‐ 95.7) 4.9 (4.7 ‐ 5.1) 8.4 (8.1 ‐ 8.6) 0.50 (0.50 ‐ 0.50) 50-54 sensitivity 4.7%, specificity 97%). < 15 99.1 (98.8 ‐ 99.3) 1.0 (0.9 ‐ 1.0) 8.4 (8.2 ‐ 8.6) 0.50 (0.50 ‐ 0.50) None of the 3 strategies performed better than chance alone in discriminating between women who did and did not have a subsequent fracture. (Crandall et al JCEM 2014) (Crandall, et al, J Clin Endocrinol Metab. 2014 Dec;99(12):4514-22. PMID: 25322268) 5
Same situation for detecting T-score ≤ -2.5 Conclusions: The FRAX threshold recommended to identify screening candidates did not identify the majority of women who subsequently experienced wrist fracture. ( J Clin Endocrinol Metab 100: 4315–4324, 2015) “fracture risk assessment tool” NOT Conclusion review [pt] Female, English language Our findings suggest that fracture risk prediction in young postmenopausal 9/25/2017 women requires assessment of risk factors not included in currently available strategies. 1. Jiang et al Obstet Gynecol 2013 117 citations 2. FitzGerald J Clin Endocrinol Metab 2014 U.S., screening or risk assessment, not 2 causes 3. Bansal Osteoporos Int 2015 6 citations 4. Crandall, et al JBMR 2014 10-years follow-up observed (incident) fractures 5. Crandall, et al, J Clin Endocrinol Metab. 2014 6. Crandall, et al, JBMR 2 citations 2015 6
Height loss Whom to screen Vertebral fractures detected incidentally by x-ray confer dx of osteoporosis. So…. √ vertebral imaging (x-ray or on DXA) if any of following: T-score Whom to treat Monitoring • ≤ -1.5 in ♀ ≥ 65-69 y/o, ♂ 70-79 y/o • ≤ -1.0 in ♀ ≥ 70 y/o ♂ ≥ 80 y/o Height loss ≥ 1.5” vs. peak, 0.8” in clinic over time - √ yearly! Low-trauma adult fx, recent/chronic prednisone use (National Osteoporosis Foundation Clinician’s Guide to Prevention and Treatment of Osteoporosis 2014) Monitoring: Measurement error Monitoring: Serial testing USPSTF Changes in BMD of < 3-6% at hip and 2-4% at spine from test to test may be Evidence is lacking about optimal intervals. due to the precision error of the test itself! Because of limitations in the precision of testing: minimum of 2 years to reliably measure a change in BMD longer intervals may be necessary to improve fracture prediction. (National Osteoporosis Foundation Clinician’s Guide to Prevention and Treatment of Osteoporosis www.nof.org 2014) (Ann Intern Med 3/1/2011) 7
Recommend



More recommend
Explore More Topics
Stay informed with curated content and fresh updates.