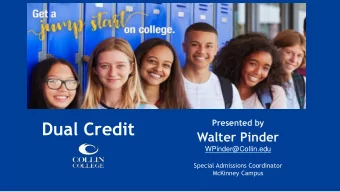
Baptist Health Quality Network Community Care Clinically Integrated Network Institutional Care • Board Primary Skilled • Payer Strategy Specialist Nursing Care & Contracting Facility Where Are We? Tertiary Committee Pharmacy Hospital • Performance Patient Centered Medical Home Improvement Governance & Quality Home Clinical Program Development Committee Long Term Health Contracting Hector Delgado, D.O. Acute Care • Professional Telemedicine Infrastructure Medical Director of Primary Care Standards • Primary Care H Collaborative Integrated Practice • Transition of Hospital ED Units Care (TOC) Hospice Payer Urgent Care Title Title 1
Title Title Physician Helpline (toll free) Physician Helpline (toll free) 1 (844) BHQN-DOC 1 (844) BHQN-DOC 1 (844) 247-6362 1 (844) 247-6362 • Providers • Physician Practice Staff • Care Coordinators • Patients Care Model • Transfer Center • Specialist • Hospital The Patient Centered Medical Home is a health care setting that facilitates partnerships between individual patients, their personal physicians and when appropriate, the patient’s family. Care is • Pharmacist • Nursing • PCP • Behavioral Health facilitated by registries, information technology, health information exchange and other means to • Psychologist assure that patients get the indicated care when and where they need and want it in a culturally • Dieticians Physician Helpline (toll free) and linguistically appropriate manner. 1 (844) BHQN-DOC 1 (844) 247-6362 We will strive for NCQA • Outpatients • Chronic certification and Joint Disease • Inpatients • BHQN Patients • Case Commission certification Managers • Non-BHQN Patients • Physician • Episodic Referral Line • Patients 2
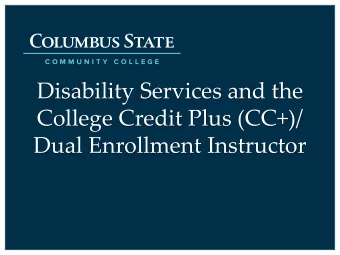
Evolution to Date Delivery of Primary Care The patient centered medical home is an approach to the delivery of primary care that is: • Patient-centered : A partnership among practitioners, patients, and their families ensures that decisions respect patients’ wants, needs, and preferences, and that patients have the education and support they need to make decisions and participate in their own care. • Comprehensive : A team of care providers is wholly accountable for a patient’s physical and mental health care needs, including prevention and wellness, acute care, and chronic care. • Coordinated : Care is organized across all elements of the broader health care system, including specialty care, hospitals, home health care, community services and supports. • Accessible : Patients are able to access services with shorter waiting times, "after hours" care, 24/7 electronic or telephone access and strong communication through health IT innovations. • Committed to quality and safety : Clinicians and staff enhance quality improvement through the use of health IT and other tools to ensure that patients and families make informed decisions about their health. NCQA- The Future of PCMH Foundation for a Better Health Care System Start-to-Finish Recognition - Before | Learn It Start-to-Finish Recognition - During | Earn It 4 1 6 7 2 3 5 8 9 Do you STOP! Transform practice Is your practice Attend free Attend free want to proceed Do you have Get the free PCMH Order free online Obtain using Standards & YES eligible for PCMH “on-board” 3 or more practice Standards & toward PCMH Standards & Guidelines application multi-site Guidelines training recognition? sites? Guidelines training recognition? approval (3-12 months) Is Is your practice eligible for As the ”textbook” for PCMH 2011 Critical training: Every practice Think you have what it takes to Order the free Online Program NO Transforming your practice into PCMH recognition?your practice recognition, the standards and considering transforming into an deliver high-quality, patient- Specific Application account. a medical home takes time. eligible for NCQA PCMH guidelines explain the NCQA-Recognized PCMH centered primary care? Move on This application will collect your Does your practice provide care Questions? Review the Multi- Training sessions The NCQA Depending on your practice’s Recognition? Before proceeding, requirements that every practice should have its engaged staff to the next step of the Start-to- information; it’s also where you at three or more sites? If so, Site FAQs and the Multi-Site PCMH Standards and current capabilities, you may consult our full eligibility criteria must meet to earn NCQA attend our free Getting on Board Finish Medical Home path to sign program agreements. you might be a Multi-Site process, Multi-site process Guidelines discuss the need 3–12 months to complete to make sure you take the right Recognition. This important training. This important 90- earn PCMH recognition. Create an account for one or Practice and could be eligible guide and additional Multi-Site requirements for earning NCQA the process and produce the path. You can also watch a video resource is available free of minute session covers the PCMH more practice sites and for for a streamlined recognition Resources. Recognition. NCQA conducts required PMCH 2011 on the important qualities of a charge recognition process from start to future Add-On and Renewal process. free, live training sessions to documentation. Although medical home. finish. Don’t start without it! Surveys. help you achieve the best NCQA evaluates your efforts, possible survey results. You we cannot provide consulting. Do you work in a specialty other can also download and listen to For a list of NCQA-Certified than primary care? If so, your a recorded training session or PCMH 2011 Content Experts, practice may be eligible for attend one of NCQA’s frequent refer to our directory. For other NCQA’s new Patient-Centered seminars across the country. questions, refer to our FAQ's. Specialty Practice Recognition You may attend as often as you program. need to. NCQA.org - Patient-Centered Medical Home Recognition NCQA.org - Patient-Centered Medical Home Recognition 3
Recommend
More recommend
Unleash a World of Digital Possibilities—Browse, Share, and Explore Content Without Boundaries