1 Annual Lower limit for Background known effects Radiation of - PDF document
Radiation Units Radiation Risks in low-Dose Imaging Grey (Gy) = amount of radiation absorbed in any material Sievert (Sv) = estimates biological effect Michael K OConnor, Ph.D. from the absorbed radiation Dept. of Radiology, Mayo Clinic
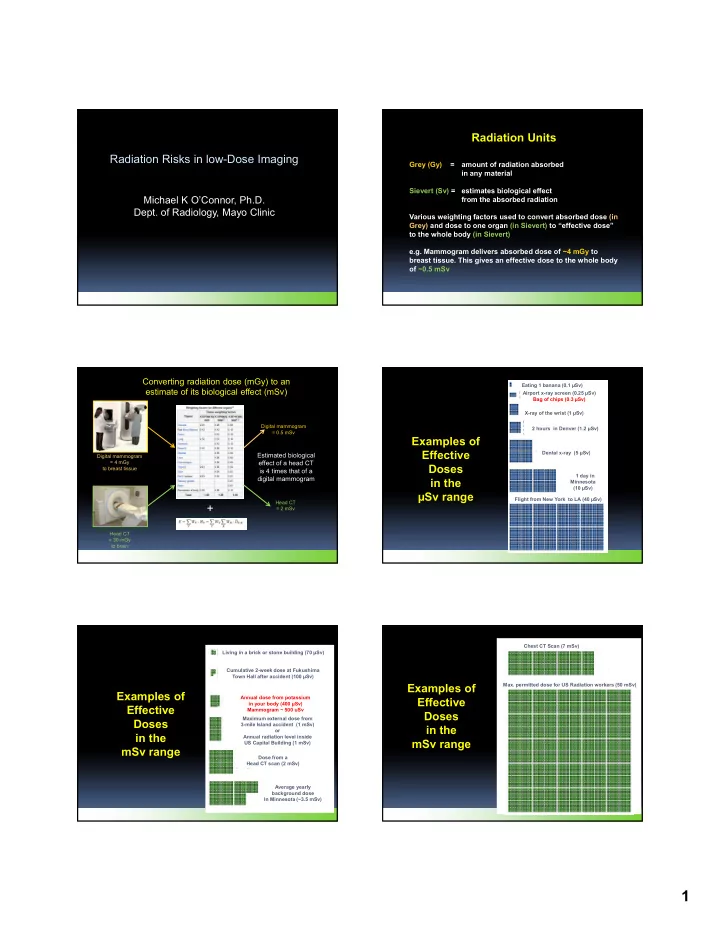
Radiation Units Radiation Risks in low-Dose Imaging Grey (Gy) = amount of radiation absorbed in any material Sievert (Sv) = estimates biological effect Michael K O’Connor, Ph.D. from the absorbed radiation Dept. of Radiology, Mayo Clinic Various weighting factors used to convert absorbed dose (in Grey) and dose to one organ (in Sievert) to “effective dose” to the whole body (in Sievert) e.g. Mammogram delivers absorbed dose of ~4 mGy to breast tissue. This gives an effective dose to the whole body of ~0.5 mSv Converting radiation dose (mGy) to an Eating 1 banana (0.1 µSv) estimate of its biological effect (mSv) Airport x-ray screen (0.25 µSv) Bag of chips (0.3 µSv) X-ray of the wrist (1 µSv) Digital mammogram 2 hours in Denver (1.2 µSv) = 0.5 mSv Examples of Effective Dental x-ray (5 µSv) Estimated biological Digital mammogram = 4 mGy effect of a head CT Doses to breast tissue is 4 times that of a 1 day in digital mammogram in the Minnesota (10 µSv) µSv range Flight from New York to LA (40 µSv) Head CT + = 2 mSv Head CT = 30 mGy to brain Chest CT Scan (7 mSv) Living in a brick or stone building (70 µSv) Cumulative 2-week dose at Fukushima Town Hall after accident (100 µSv) Examples of Max. permitted dose for US Radiation workers (50 mSv) Examples of Annual dose from potassium Effective in your body (400 µSv) Effective Mammogram ~ 500 uSv Doses Maximum external dose from Doses 3-mile Island accident (1 mSv) in the or in the Annual radiation level inside mSv range US Capital Building (1 mSv) mSv range Dose from a Head CT scan (2 mSv) Average yearly background dose In Minnesota (~3.5 mSv) 1
Annual Lower limit for Background known effects Radiation of radiation Lowest 1-year dose clearly linked to increased cancer risk (100 mSv) Examples of Severe radiation poisoning, in some Effective cases fatal (2000 mSv) Doses No reliable Known ? data on detrimental carcinogenic Fatal dose, even with treatment (8000 mSv) in the effects of radiation effects Sv range Very Low low dose dose range range Radiation Dose (mSv) Radiation is a poor carcinogen ! Risk Estimates require “Impracticably Large” sample requirements Does the radiation from mammography (about 1 mSv) cause breast cancer? Cohort study: about 100 million (20-year follow-up)! Case-control: about 1 million cases (4:1 ratio) 9 10 Why are we concerned with Radiation Risks? Sample size required to detect a significant increase in cancer mortality, assuming lifetime follow-up Required number of subjects in study Dose range of relevance for radiology) Using LNT & BEIR VII report, estimated radiation-related incident cancers Estimated that 29,000 future cancers could be related to CT scans performed in the U.S. in 2007…..and would translate into about Dose (mSv)) 14,500 cancer deaths. National Research Council (1995) Radiation Dose Reconstruction for Epidemiologic Uses (Natl. Acad. Press, Washington, DC). Arch Intern Med. 2009;169(22):2078-2086 2
Consequences: Heightened fear of radiation = Negative impact on care Patients declining needed exams or procedures Physicians ordering alternate exams, which may be less accurate or more expensive Where does the estimate of 29,000 cancers Radiophobia come from ? Fukushima The number of deaths indirectly related to the earthquake in Fukushima Prefecture was >1700 . Based on BEIR VII + Deaths were due to the risk estimates for physical / mental stresses 56,900,000 patients related to the evacuation. What is the BEIR VII Report An estimate of cancer risk from low doses of ionizing radiation! Sources of data Input data: Environmental studies Occupational studies • Environmental Radiation Studies Medical studies Atomic bomb studies • Occupational Radiation Studies Risk models (based on above input data): ERR (excess relative risk) • Medical Radiation Studies EAR (excess absolute risk) LAR (lifetime attributable risk) • Atomic bomb survivor Studies Subjective opinion of committee ! Linear No Threshold hypothesis Latency period / DDREF 3
Cancer Mortality in High Background Radiation Area of Sources of data used in BEIR VII Yangjiang, China, 1979-1995 Environmental Radiation Studies Estimated cancer risk Populations living near nuclear facilities associated with the low level “..no increased risk…with radiation exposure” radiation exposure of 6.4 mSv / year Populations exposed to atomic bomb testing 20-year study in 125,079 “..some studies (4 out of 10) show some effect” subjects Chernobyl Excess Relative Risk High incidence of thyroid cancer ERR/Sv = -0.10 (-0.67 to 0.69) “..no evidence of an increase in any solid cancer type to date” Conclusion: the mortality of all cancers in Yangjiang was Natural background (China / India) generally lower than that in “..did not find higher disease rates in geographical areas control group, but not with high background levels..” significant statistically. (Tao et al, Zhonghua Yi Xue Za Zhi, 1999; 79: 487-492) Radon Levels Lung Cancer Sources of data • Environmental Radiation Studies • Occupational Radiation Studies • Medical Radiation Studies Generated from EPA web site Generated from NCI mortality map • Atomic bomb survivor Studies (https://www.epa.gov/radon/find- (http://ratecalc.cancer.gov/ratecalc/) information-about-local-radon-zones- and-state-contact- information#radonmap) Occupational Radiation Studies on Workers in Sources of data the Nuclear Power Industry “….in most cases, rates for all causes and all • Environmental Radiation Studies cancer mortality in the workers were substantially lower than the reference • Occupational Radiation Studies populations.” • Medical Radiation Studies Findings explained as “healthy worker effect” (U.S. Academy of Science, BEIR VII, 2007) • Atomic bomb survivor Studies Significant limitation of most occupational studies is absence of an appropriate control group ! 4
Mortality from Breast Cancer after Fluoroscopy Medical Radiation Studies in Patients being treated for Tubercolosis 31,710 women treated between 1930 - 1952 40-year follow-up Sources of data used in BEIR VII Age range 10-40 years Standardized Death Rate / 10 6 py Focus on therapeutic studies “Risk was statistically significant for all those “…most of the information comes from studies who received more than 100 mSv of radiation” of populations with medium to high doses” Lung Cancer – 9 studies, 40,000 subjects average dose ~ 1 Gy Breast cancer – 11 studies, 20,000 subjects average dose ~ 300 mGy Dose (mSv) Miller AB et al, NEJM 1989; 321: 1285-1289. Atomic bomb survivor Studies Sources of data used in BEIR VII • 120,000 survivors 93,000 present at time of bombings 27,000 from locale, but absent at time • Environmental Radiation Studies of the bombing (Not In City group) • Occupational Radiation Studies • Monitored over 70 years & includes both sexes and all ages of exposure – mean dose = 200 mSv • Medical Radiation Studies • Dose range 37,000 0-5 mSv 32,000 5-100 mSv • Atomic bomb survivor Studies 17,000 100 mSv – 2000 mSv This is the primary source of data for LNT risk models Atomic bomb survivor Studies Atomic bomb survivor Studies Data from Table 4, Data from Table 4, Preston et al, 2007 Preston et al, 2007 # solid cancers # solid cancers adjusted to per adjusted to per Radiology 100,000 people 100,000 people Preston et al, Rad Res 2007;168: 1-64. Preston et al, Rad Res 2007;168: 1-64. (Radiation Effects Research Foundation) (Radiation Effects Research Foundation) 5
Atomic bomb survivor Studies – 70 yrs follow-up Risk Models used in BEIR VII Ozasa et al, 2013, Doss et al 2012 Risk models are generated from high-dose studies ! Radiology Excess Relative Risk (ERR) model The ERR is the rate of disease in an exposed population divided by the rate of disease in an unexposed population, minus 1.0. Excess Absolute Risk (EAR) model The EAR is the rate of disease in an exposed population minus the rate of disease in an unexposed population. Risk Models used in BEIR VII Same Data – 2 different Risk Models Comparison of Lifetime Risk of Cancer using ERR and EAR Excess Relative Risk (ERR) 800 vs. Males Females 700 Excess Absolute Risk (EAR) Breast 600 LAR based on ERR Model 500 Which model is correct ? 400 Stomach 300 For each organ, final risk model 200 = x.ERR + (1-x).EAR 100 where x is determined by committee ! Prostate 0 0 100 200 300 400 500 600 700 800 LAR based on EAR Model Effect of Low Doses - 3 Hypotheses Linear No-Threshold Hypothesis Linear No Threshold (LNT) Model LNT & Radiation Threshold Model • 1930’s: developed by Herman Mueller to explain Hormesis Model mutagenesis in fruit flies • 1950: Mueller persuaded BEIR committee in 1950 to use his LNT hypothesis to explain carcinogenesis LNT assumes that LNT any amount of radiation exposure, no matter how small, can increase the chance of cancer. Hormesis probability of cancer from radiation exposure increases with cumulative lifetime dose. 6
Recommend








More recommend
Explore More Topics
Stay informed with curated content and fresh updates.